ENDOCRINE SYSTEM
Parathyroid and thyroid
Figure 12.24 provides a ventral view of the ferret head and neck region and shows the position of the thyroid and parathyroid glands plus the right medial retropharyngeal lymph node.
The latter can be the site of neoplasia, as can other external lymph nodes. The ventral isthmus of the bilobed thyroid lies dorsal to the tracheal rings. The thyroid is darker than the pale parathyroid glands, which lie cranial to it along the trachea.Adrenal glands
The adrenal glands and the pancreas have been sites of increasing numbers of neoplasia in ferrets in recent years.
The left and right adrenal glands (Fig. 12.16) are situated adjacent to the upper borders of the left and right kidneys and are usually embedded in fat. The exact positions vary with individual animals (Holmes 1961). Both adrenal glands are subject to hormone-stimulated neoplasia. The left adrenal gland is found close to the left side of the abdominal aorta and caudal to the origin of the cranial mesenteric artery. The gland measures 6-8 mm, is oval-shaped and usually of a pinkish color. It may also have a grooved surface due to the adrenolumbar vein, which crosses it to enter the vena cava.
The right adrenal gland is more elongated (approximately 8-11 mm long) and is in a more dangerous position in relation to possible surgery. It lies more rostral than the left gland, being close to the point of origin of the cranial mesenteric artery. It should be noted that the right adrenal gland is always related ventrally to the caudal vena cava, which may overlap the medial half of the gland or overlie it completely. The right adrenal gland may also be grooved by the right adrenolumbar vein.
The adrenal glands have been well documented by Holmes (Holmes 1961). Their anatomical placing makes a complete adrenalectomy operation difficult. Their blood supply is basically via vessels from the renal artery and vein and cranial mesenteric artery, though Holmes found variations.
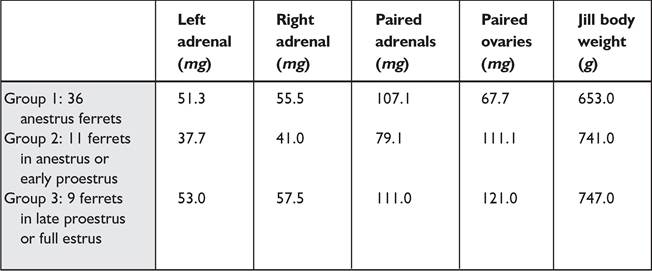
In structure, the adrenal cortex has three main zones, as seen in other animals: the glomerulosa, fasciculata, and reticularis plus the zona intermedia and zona juxtamedullaris (Holmes 1961).Holmes has given an idea of adrenal gland and ovary size in relation to jill body mass. Ferrets in late proestrus or full estrus show an adrenal mass increase (Table 12.2).
Hormonal disorder of the adrenal gland, which is not associated with the pituitary gland, is the overproduction of various sex hormones leading to unilateral or bilateral hyperplasia, adenomas or adenocarcinoma. It is theorized that in the embryonic stage, the ovaries and adrenal glands develop in the same embryonic region and, possibly, some ovarian cells are taken up by the adrenal gland and become part of the outer cortex (Rosenthal 1997). Some stimulation leads to excess sex hormones (especially estradiol) being released and affecting the ferret physiology, male or female (Table 12.3).
The primary clinical sign of AGN is alopecia, gradually affecting the whole body. It is at epidemic levels in pet ferrets in the USA, with incidences rising from 30% in 1993 to 70% in 2003. Approximately 80-90% of cases are unilateral (Finkler 2002). The average age of American ferrets when affected is 3½-4½ years but it has been seen in ferrets from 8 months to 9 years. Additional signs include lethargy and muscle atrophy, pruritus in the jill with vulval swelling, vaginitis, and stump pyometra. In hobs the prostate is affected, showing enlargement and stranguria. Diagnosis is usually on clinical signs and history.
The history (etiology) of affected American pet ferrets is interesting. Basically, they are sterilized at 6 weeks of age, kept in apartments or houses under unnatural lighting and for extended photoperiods. This contrasts to Australian ferrets,
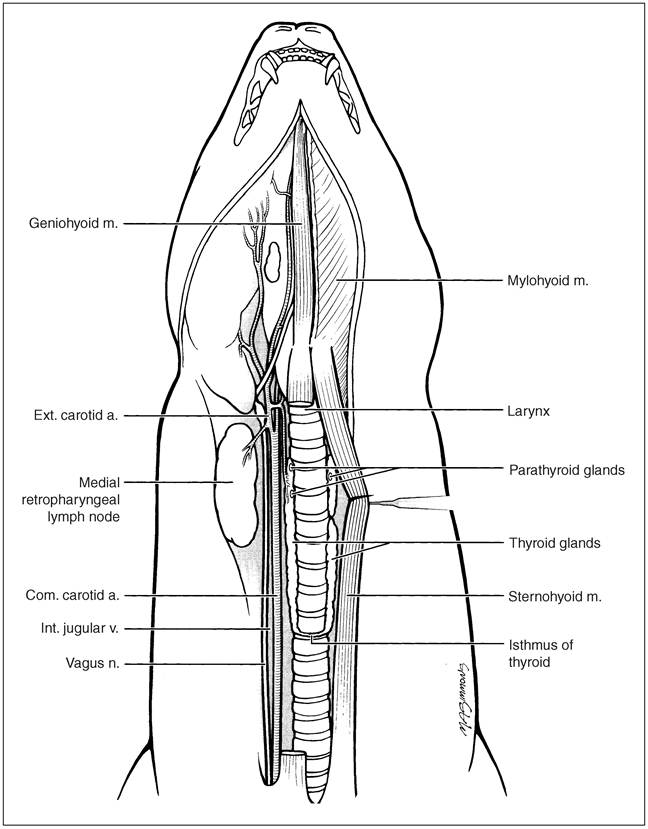
Figure 12.24 • Ferret endocrine glands. (Courtesy of Howard Evans.)
which are sterilized at 5-6 months of age and kept outside in cages or in an enclosed “ferret-proof” garden or ferretarium arrangement (Lewington 2003a).
In the case of ferrets it is surmised that early sterilization stimulates the growing adrenal glands to produce sexual
hormones in an unnatural position in the body, without the normal negative feedback mechanism of estrogens and androgens on the hypothalamus. The proposed scenario is that the hypothalamus continues to secrete gonadotropin-releasing hormone (GnRH). This gives a continuous stimulation for
Table 12.2 Adrenal gland and ovary weights in the ferret
| Table 12.3 Estrogen precursor values in normal and AGN affected ferrets | ||
| Steroid | Normal ferrets | AGN ferrets |
| Androstenedione (nmol/L) | 6.6 | 67 |
| DHEAS (mol/L) | 0.01 | 0.03 |
| Estradiol (mol/L) | 106 | 167 |
| 17-Hydroxyprogesterone (nmol/L) | 0.4 | 3.2 |
DHEAS, Dehydroepiandrosterone sulfate
After Rosenthal, K. (1997) In E. V. Hillyer & K. E. Quesenberry (eds.), Ferrets, rabbits and rodents: Clinical medicine and surgery. Philadelphia: WB Saunders, with permission.
the pituitary gland to secrete luteinizing hormone (LH) and follicle-stimulating hormone, (FSH), which in turn stimulate the incorporated ovarian cells in the adrenal gland cortex.
American veterinarians agree that the unnatural photoperiods (living under artificial light) combined with early desexing are predisposing pet ferrets to the disorder. Ferrets are highly sensitive to the photoperiod; unspayed jills are sexually controlled by it. Melatonin is the hormone produced in the dark by the pineal gland; it has been implicated in a wide range of physiologic processes, including reproduction (through its effects on gonadotrophins).
Melatonin levels normally increase as the photoperiod decreases. In humans melatonin is considered anticancer. The photoperiod of “in house” pet ferrets is largely determined by artificial lighting and rarely mimics the natural period. Thus, not only are these ferrets subject to abnormally long (or short) photoperiods but there is often a lack of normal seasonal fluctuation. The abnormal melatonin secretion could therefore affect the adrenal gland. Possibly melatonin could be given orally to pet ferrets to prevent the disease but it has only a short action and there is no injectable form as yet (Finkler 2002).Treatment is either surgical or long-term medication with drugs, many of them human ones and expensive. Surgery for a unilateral AGN case in my own pet ferret has been described (Lewington 2003e) while Bennett describes surgery for a complex bilateral AGN case (Bennett & Pye 2000). Medication without surgery has been described (Finkler 2002; Lewington 2003e) and work on the disease is ongoing in the USA. Actually, AGN cases will live for over a year post-diagnosis without treatment, until complications occur.
The pancreas
The organ is ‘v'-shaped, elongate and lobular, being light pink to bright red on surgical examination. It consists of right and left limbs (lobes) associated with the central mass adjacent to the pylorus (Fig. 12.25). The left limb, shorter than the right, runs along the visceral surface of the stomach with the spleen lateral. It is bi-angular in cross-section and enclosed in the mesoduodenum. Dorsally, it is near the portal vein, left kidney, and left adrenal gland. The right limb (see Fig. 12.15a) follows the descending part of the duodenum on the dorsomedial aspect.
Whereas AGN can be cured, to some extent, insulinoma, a condition of the pancreas, is not and is another ongoing medical problem for mostly American pet ferrets (Fig. 12.26). Raised nodules of pancreatic islet cells over the surface of the organ indicate insulinoma in the ferret.
Insulinoma is primarily found in American pet ferrets where small tumors of the pancreatic islet cells produce a high level of insulin, which can be fatal in producing hypoglycemia due to blood-sugar depression. Thus the normal feedback mechanism, to stabilize the animal with low blood sugar, is compromised by the neoplastic cells. Interestingly, in early cases there is some stimulation of liver gluconeogenesis and glycogenolysis, but the process becomes inefficient. Blood-sugar depletion affects brain function, with deprivation of energy source and resulting dullness and confusion (Quesenberry 1997). Clinical signs of the condition are hind leg weakness and a tendency for the ferret to stare blankly into space and drool excessively. Hypoglycemia leads to seizures and death.
The feeding of ferrets on high carbohydrate, high fiber (processed) foods, as distinct from a natural diet, are thought to be an etiological cause. Ad libitum feeding of in-house ferrets with dry foods will add to the problem. Ferrets should have a high protein, high fat (for energy), low carbohydrate and low fiber diet, and be fed no more than twice daily. General ideas on feeding ferrets have been described (Lewington 2003b).
Treatment of insulinoma is by surgery (Bennett & Pye 2000) and requires special postoperative care (Lewington 2003f). Affected treated ferrets can live for 1-3 years but require owner patience and attention. In AGN and insulinoma prevention is better than cure.
KEY NOTES
• Early neutering and lack of a natural photoperiod may predispose a ferret to adrenal gland neoplasia (AGN).
• The left adrenal gland is more accessible for surgery than the right because the right adrenal is intimately associated with the caudal vena cava.
• The pancreas is commonly a site of insulinoma.