Exchange of Oxygen and Carbon Dioxide Between the Alveolus and Pulmonary Capillary Blood Occurs by Diffusion
Diffusion is the passive movement of gases down a concentration (partial pressure) gradient. The rate of gas movement between the alveolus and the blood (Vo2) is determined by the physical properties of the gas (D), the surface area available for diffusion (A), the thickness of the air-blood barrier (x), and the driving pressure gradient of the gas between the alveolus and capillary blood (PAo2 - Pcapo2), as follows:

D is determined by several factors, including the molecular weight and solubility of the gas.
The alveolar surface area (A)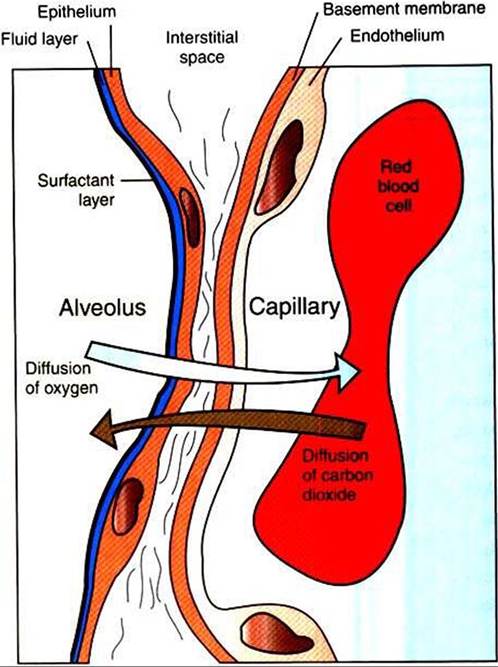
FIGURE 47-2 Diagrammatic representation of the airblood barrier within the lung, showing the pathway for diffusion of oxygen and carbon dioxide between the alveolus and the erythrocyte within the pulmonary capillary.
available for diffusion is that occupied by perfused pulmonary capillaries. During exercise, more capillaries become perfused by blood, and thus the surface area available for diffusion increases.
In the lung the barrier separating air and blood is less than 1 μm thick (Figure 47-2). However, although thin, this barrier includes a layer of liquid and surfactant lining the alveolar surface; an epithelial layer, usually formed by type I epithelial cells; a basement membrane; variable-thickness interstitium; and a layer of endothelium. In addition to moving gases through this air-blood barrier, diffusion also moves gases within the plasma, allowing oxygen to gain access to erythrocytes and hemoglobin.
Blood entering the alveolar capillary from the small pulmonary arteries is known as mixed venous blood because it is blood that has returned to the right side of the heart in veins from all parts of the systemic circulation.
The driving pressure for gas diffusion is the difference in oxygen tension between the alveolus and the capillary blood. PAo2 averages IOO mm Hg; in a resting animal, blood entering the alveolar capillary—that is, mixed venous blood—has an oxygen tension (Pvo2) of approximately 40 mm Hg. The driving pressure gradient of 60 mm Hg (100-40) causes rapid diffusion of oxygen into the capillary, where it combines with hemoglobin. Hemoglobin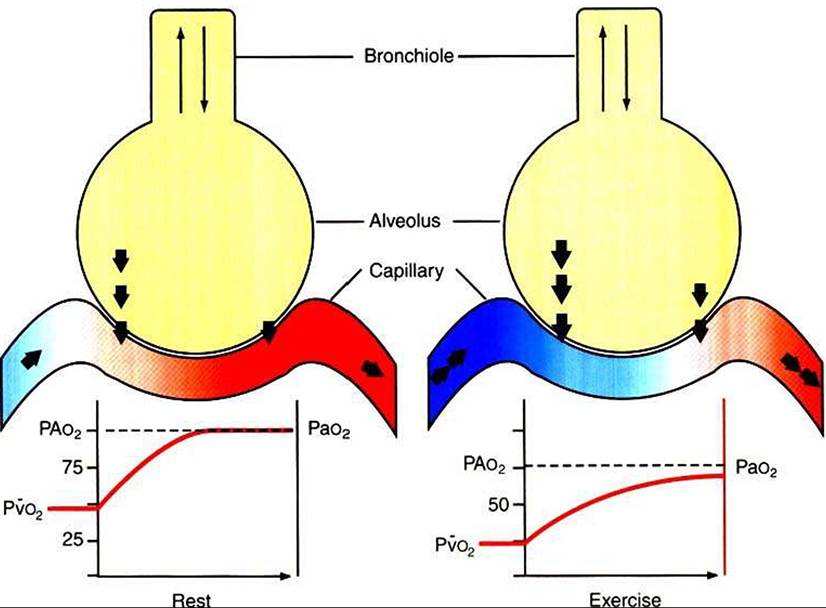
FIGURE 47-3 Schematic representation of alveolus and pulmonary capillary, showing the increase in oxygen (Po2) tension that occurs as blood passes through the capillaries. The shaded area within the alveolus represents mixing of gases by diffusion. The size of the arrows between the alveolus and the capillary represents the magnitude of the oxygen fluxes. In the resting animal, mixed venous oxygen tension (Pvo2) is approximately 40 mm Hg, and blood and air equilibrate rapidly. In the exercising animal, mixed venous oxygen tension is low, and even though oxygen fluxes are high, the blood has not equilibrated with the alveolar oxygen tension before it leaves the alveolus.
PAo2, Alveolar oxygen tension; Pao2, arterial oxygen tension.
takes up oxygen from the plasma and helps maintain the gradient for oxygen diffusion.
Normally, equilibration between alveolar and capillary oxygen tensions occurs within 0.25 second, approximately one third of the time the blood is in the capillary (Figure 47-3). During strenuous exercise, muscles extract a large amount of oxygen from the blood, so the mixed venous blood returning to the lung contains little oxygen. In addition, during exercise the cardiac output is high, and the velocity of blood flow through the capillaries is rapid. More oxygen must therefore be transferred in less time than in the resting animal. Under these strenuous conditions, diffusion equilibrium may not occur, and the oxygen tension of blood leaving the lung and entering the systemic arteries (Pao2) may decrease during intense exercise.
This exercise-associated hypoxemia is observed in racing Thoroughbred horses.In a diseased lung, diffusion of oxygen may be impeded as a result of inflammation and edema, which may thicken the air-blood barrier or reduce the surface area available for gas exchange. In these situations the therapeutic administration of oxygen can increase PAo2 and thereby provide a greater driving pressure to deliver oxygen into the blood.
The carbon dioxide tension of venous blood returning to the lungs averages 46 mm Hg, and alveolar carbon dioxide tension (PAco2) is 40 mm Hg. Thus the driving pressure for diffusion of carbon dioxide is only 6 mm Hg. Despite this small driving pressure, the amount of carbon dioxide that diffuses per minute between the capillaries and the alveoli is similar to the amount of oxygen. The 20-fold greater solubility of carbon dioxide compared with oxygen compensates for the small driving pressure gradient. For the same reason, carbon dioxide diffusion between the blood and the alveoli is rarely affected by lung disease.