EXTERNAL EAR
The external ear consists of the external auditory canal and its cartilaginous extension, the auricle (pinna). The auricle, sometimes known as the ear leather to dog fanciers, is shaped like a lopsided funnel, with a

Figure 11-40 Erect posture of the external ears.
small cutaneous pouch on the caudal border a short distance above the ear opening (Figure 11-40 and Figure 11-41). There is a wide diversity in the shape, size, and posture (erect or folded) of dog ears. It is not clear if this diversity influences the hearing ability. Most cats have erect auricles, but an exception is the Scottish Fold cat, in which the most distal portion of the auricle bends rostroventrally, beginning at 3 to 4 weeks of age.
The basis of the auricle is a plate of fibroelastic cartilage that is covered by subcutaneous tissue and skin.
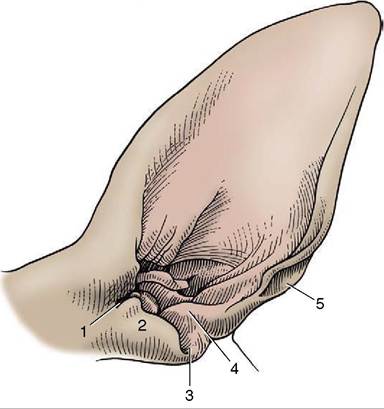
Figure 11—41 Left canine ear, shaved. 1, Pretragic notch;
2, tragus; 3, intertragic notch; 4, antitragus; 5, cutaneous pouch.
The skin on the inner (concave) surface adheres more firmly to the cartilage than that on the outer part.
The features of the auricular cartilage provide important surgical landmarks known as the helix, antihelix, tragus, antitragus, and scapha (see Figure 11-41).
The tragus forms the lateral rim of the ear canal opening; it is separated from the more caudal antitragus by the intertragic notch. Both consist of rolled up articular cartilage that supports the external ear opening. The antitragus forms the caudal part of the ear opening and ascends toward the end of the lateral side.
The proximal part of the auricular cartilage is rolled to form a partial tube called the concha, which serves as the enlarged entry of the auditory canal.
This first part of the canal connects to the short annular cartilage, which terminates in a short osseous external canal. The ear canal is first directed ventrally (auricular cartilage) before turning medially to form the horizontal canal (portion of the auricular and annular cartilages), which is surrounded and supported by the temporal bone. This course hampers passage of the straight otoscope for examination of the proximal part of the canal and the eardrum. The canal must be straightened by pulling the ear first caudally, then ventrally as the otoscope is advanced (Figure 11-42). The canal is about 7 cm long.The horizontal ear canal ends at the eardrum. The tympanic membrane consists of an outer epithelial layer, which is a continuation of the skin of the external auditory canal, an inner mucosal layer, and a fibrous layer in between. The tympanic membrane is thin, slightly oval, semitransparent, and concave owing to traction on its medial side by the tensor tympani muscle.
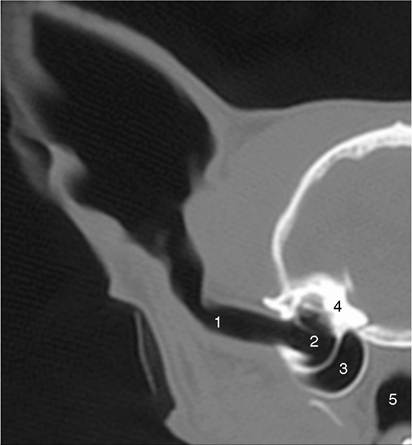
Figure 11—42 Transverse CT scan (bone window) of half of a feline head showing ear canal and middle ear. 1, Ear canal; 2, tympanic cavity; 3, tympanic bulla; 4, petrous temporal bone; 5, nasopharynx.
The appearance of the tympanic membrane (eardrum) through an otoscope is shown in Figure 11-43, A-B. The tympanic membrane consists of a small upper portion, the pars flaccida, and a large lower portion, the pars tensa (thin, tough, and glistening). The outline of the manubrium of the malleus is clearly visible.
The auricular skin continues as the lining of the auditory canal. This skin is thin, and its lateral part possesses both ceruminous and sebaceous glands. It generally contains only a few hairs, but in some breeds (Poodles) hair is abundant. The skin of the bony part of the ear canal is much thinner than that of the cartilaginous portion and is continuous with the epithelial layer of the tympanic membrane.
There are no glands or hair follicles here where, because of its thinness, it is more sensitive to trauma.The base of the auricle and the ear canal are related laterally and ventrally to the parotid gland. The facial nerve crosses the ventral surface of the canal deep to the gland before breaking into the auriculopalpebral nerve and the two buccal branches. The former passes dorsally in front of the ear with the superficial temporal vessels. This stretch of the facial nerve also detaches a caudal auricular nerve and a branch to the middle ear. The sensory innervation is provided by the trigeminal, glossopharyngeal, vagus, and second cervical nerves. The innervation of the muscles of the external ear is by the facial nerve.
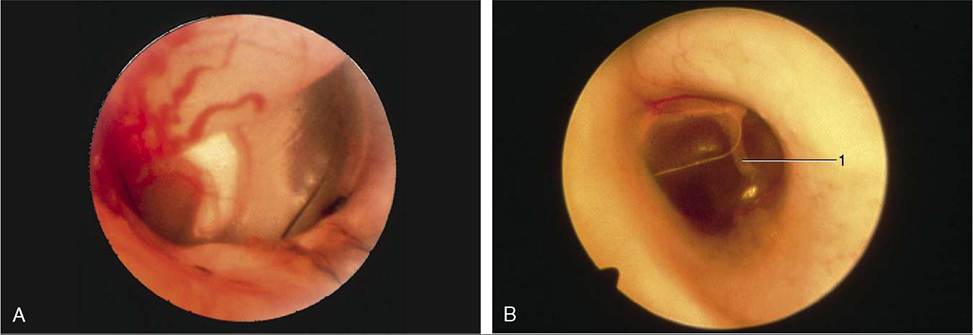
Figure 11—43 A, Otoscopic view of eardrum showing handle of malleus. B, Otoscopic view of the ear drum (cat). 1, Malleus.
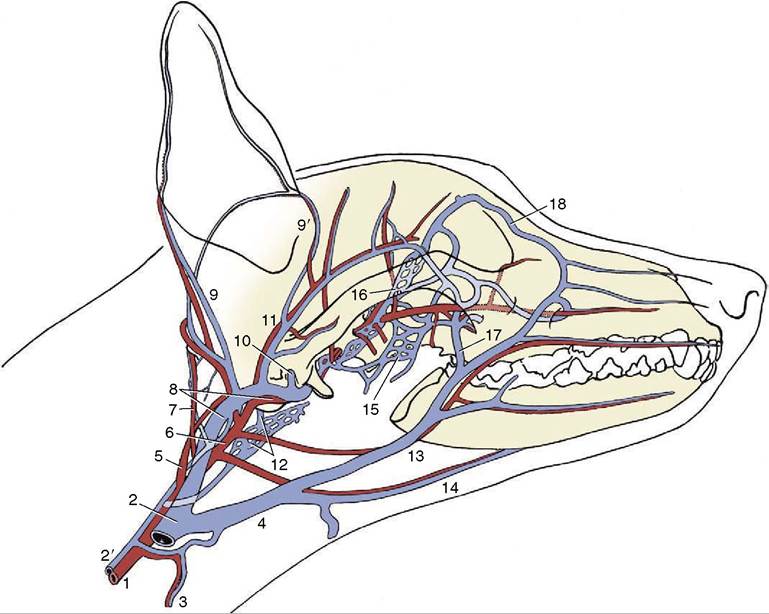
Figure 11-44 The major arteries (red) and veins (blue) of the canine head. The ramus of the mandible has been removed. 1, Common carotid; 2, external jugular; 2', internal jugular; 3, cranial thyroid; 4, linguofacial; 5, internal carotid; 6, external carotid; 7, occipital; 8, maxillary; 9, 9', caudal and rostral auricular; 10, dorsal emissary; 11, superficial temporal; 12, ventral emissary and pharyngeal plexus; 13, facial; 14, lingual; 15, pterygoid plexus; 16, ophthalmic plexus; 17, deep facial; 18, angularis oculi.
The veins of the area join the maxillary vein, which descends toward the mandibular gland from its formation by substantial caudal and cranial auricular and superficial temporal veins that may pass through the parotid gland (Figure 11-44).
The arteries lie more deeply. The external carotid having detached the caudal auricular artery to the convex surface of the auricle ends rostroventral to the ear canal by dividing into maxillary and superficial tem- poraral arteries. The latter, with the like-named vein, lies deep to the parotid gland close to the rostral surface of the ear canal.
The caudal auricular artery branches in the convex outer surface of the auricle; it sends finer branches to the skin over the concave surface through small holes in the cartilage. Vigorous and repeated head shaking or scratching, in most instances elicited by parasites or infection of the ear canal, may injure the vessels and cause hematomas by rupture of the penetrating small branches. Because the hematoma is lined by cartilage on both sides, splitting of the auricular cartilage also takes place. Once begun, the bleeding between the cartilages continues until the internal pressure equals the pressure in the feeder arteries.