Facial expression
Key points
■ Muscles of facial expression are innervated by the motor nucleus of CN VII sited in the rostral medulla oblongata.
■ The facial nucleus receives inputs for reflex function from other brainstem nuclei and from the cerebrum for facial expression.
The location of the motor nucleus of CN VII is in the ventrolateral area of the rostral medulla oblongata (see Fig. A29). Afferents to the facial nucleus are used in protective functions involving facial musculature. Examples include, afferents from the spinal nucleus of CN V (trigeminofacial and corneal reflexes - for facial or eyelid movement after a sensory stimulus) and the trapezoid body and cochlear nuclei (acousticofacial reflexes such as closing the eyes after a loud noise). There is also input from the cerebral cortex (via the corticonuclear tract) for controlling facial expression. From the facial nucleus, the efferent fibres pass dorsorostromedially to loop around the abducens nucleus (CN VI) and then descend to exit the brainstem ventrolaterally. This loop is called the internal genu of the facial nerve. The neurons of the nucleus are topographically arranged so that rostral neurons innervate rostral muscles, caudal neurons supply caudal muscles, but dorsal neurons innervate ventral muscles and vice versa. The facial nerve exits the neurocranium via the internal acoustic meatus and passes through the facial canal in the petrosal portion of the temporal bone. The portion of this canal that lies adjacent to the tympanic cavity of the middle ear lacks a bony wall, and the nerve is separated from the cavity by only a few micrometres of loose connective tissue. Thus lesions in the middle ear may cause dysfunction of CN VII. Once it emerges from the stylomastoid foramen at the base of the external ear canal, it branches and the buccal branches run superficially across the masseter muscle and is often palpable in the intact animal. Its superficial path makes it vulnerable to trauma and pressure such as from harness buckles (see Figs. 10.14 and 13.2). Facial nerve dysfunction results in loss of facial and auricular movement and muscle tone. With unilateral lesions, there is loss of facial symmetry (Fig. 10.14).
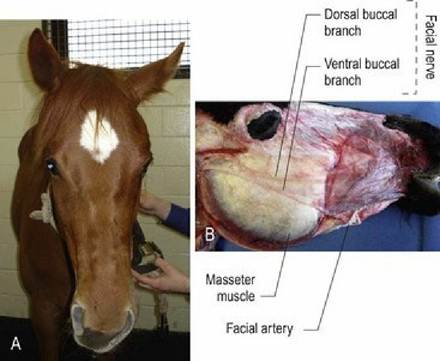
Fig. 10.14 (A) Left-sided facial paresis secondary to otitis media. (B) Superficial dissection of a horse’s face to display the superficial portions of the facial nerve
(photo courtesy of Mr. Allan Nutman, Massey University).