FATE OF ERYTHROCYTES
1. What cell accounts for removal of about 90% of aged RBCs? What are the organs where this occurs?
2. How can icterus (jaundice) occur during the degradation of hemoglobin?
3.
How can hemoglobinemia and hemoglobinuria occur as a result of RBC destruction?As erythrocytes age, several metabolic changes occur: the membrane becomes more rigid and fragile, and the discocyte converts to a poorly deformable spherocyte. Accordingly, some intravascular hemolysis of erythrocytes occurs (10%) and the remainder of the aged RBCs (about 90%) is selectively removed from the circulating pool by cells of the MPS, mostly by the fixed cells in the spleen, liver, and bone marrow.
When erythrocytes are phagocytized by MPS cells, they undergo hemolysis within the phagocytic cell (extravascular or intracellular hemolysis), and the Hb, other proteins, and membrane lipids of the phagocytized RBCs are catabolized. A summary of Hb degradation that begins in this way is shown in Figure 3-9. The iron and globin are separated from heme, globin is degraded to its amino acids, and both iron and globin amino acids are reutilized. Iron is stored in the MPS cells in the form,of ferritin and hemosiderin or is transferred to plasma, where it combines with a plasma protein, apotransferrin, to become transferrin. Transferrin circulates to the bone marrow, where the iron is used for the synthesis of new hemoglobin. During Hb synthesis, iron released from decomposing RBCs is used in preference to storage iron.
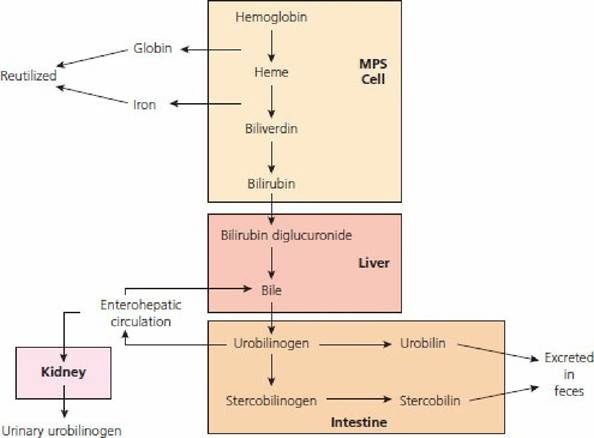
■ FIGURE 3-9 Degradation of hemoglobin that began within mononuclear phagocytic system (MPS) cells. Iron released as shown is used preferentially for synthesis of new hemoglobin. Protein (globin) is degraded to amino acids and reutilized. Bilirubin released from MPS cells is insoluble and combines with a protein (known as free bilirubin) and is transported to the liver, where it is converted to bilirubin diglucuronide (soluble form of bilirubin).
The soluble form enters the biliary system and is transported to the intestine. Bacterial reduction of bilirubin diglucuronide produces urobilinogen, which may be recirculated via the enterohepatic circulation or further reduced to urobilin or stercobilinogen. Some of the recirculated urobilinogen bypasses the liver, enters the general circulation, and is excreted in the urine. (From Reece WO, Swenson MJ. The composition and functions of blood. In: Reece WO, ed. Dukes’ Physiology of Domestic Animals. 13th edn. Ames, IA: Wiley-Blackwell, 2015.)Heme is converted to biliverdin (a green pigment) and then reduced to bilirubin (a yellow pigment). Free bilirubin (water-insoluble) is released into the plasma, where it becomes bound to albumin (a plasma protein) and transported to the liver and.“dumped.” In the liver, the insoluble bilirubin conjugates with glucuronic acid to form bilirubin glucuronide, mainly diglucuronide, which is watersoluble. It is secreted into the bile in this form and enters the intestine. Bacteria within the large intestine reduce bilirubin diglucuronide to urobilinogen. Most urobilinogen is excreted with the feces in the oxidized forms of urobilin or stercobilin, which are pigments that give feces its normal color. Part of the urobilinogen is reabsorbed into the enterohepatic circulation, from which most is reexcreted into the bile. Some of the absorbed urobilinogen bypasses the liver, enters the general circulation, and is excreted in the urine to become a part of the normal pigment of the urine as urobilin. Carbon monoxide (CO) is formed when the porphyrin ring of heme is opened. This is the only reaction in the body in which CO is formed and is excreted by the lungs.
Because of liver disease, free bilirubin combined with albumin might not be “dumped” and would continue to circulate and appear in high concentrations in the plasma and interstitial fluids. Also, if the bile duct becomes blocked, the bilirubin glucuronides (soluble bilirubin) could spill over into the plasma. Both of these conditions can produce a yellow color in the tissues known as icterus, or jaundice.
When erythrocytes are hemolyzed intravascularly, the Hb is first bound to haptoglobin (a plasma protein). This complex is rapidly removed by cells of the MPS and the Hb is degraded as described above for extravascular hemolysis. Because the complex is a large molecule, it is not filtered through the kidney glomeruli. However, excessive intravascular hemolysis (hemolytic disease) can occur and sufficient haptoglobin might not be available. The plasma takes on a reddish appearance and the condition is known as hemoglobinemia. The free Hb is then filtered at the glomeruli and enters the kidney tubules. Much of it is reabsorbed from the tubules, but can surpass the renal threshold for reabsorption and continue into the urine to give it a reddish color, a condition known as hemoglobinuria.
■