Fetal Circulation
Throughout gestation, the fetus depends on the dam for the nutrients, water, and oxygen needed for growth and for the elimination of carbon dioxide and other waste products of fetal metabolism.
During fetal development, the lungs are collapsed and not aerated, and the pulmonary vascular beds have high resistance to blood flow. The fetal circulation therefore bypasses these pulmonary capillary beds. Immediately after birth, however, the newborn needs to direct its blood through the pulmonary vessels for oxygenation. The heart and circulatory system are arranged in such an ingenious way that the cardiopulmonary circulation just moments after birth is profoundly different from that exhibited just prior to the first breath (Fig. 17-10).Because it is exchanging gas, supplying nutrients, and removing metabolic waste products, the placenta must necessarily receive a large proportion of the fetus’s circulating blood.
It does so via two large umbilical arteries, extending from the caudal end of the abdominal aorta through the umbilical cord to the placenta. After passing through the placental capillary bed, the blood is returned to the fetus by a single umbilical vein, which passes into the substance of the liver. Most of the highly oxygenated blood returning from the placenta in the umbilical vein is delivered directly into the caudal vena cava, bypassing the hepatic sinusoids via a fetal diversion, the ductus venosus.
Two features of the fetal heart allow blood to bypass the pulmonary circulation. During cardiogenesis, the wall between the two atria develops a flutter valve. This aperture is called the foramen ovale, and its structure is such that the blood entering the right atrium (well oxygenated, as a goodly portion of it is returning from the placenta) uses the one-way flutter valve of the foramen ovale as a convenient passageway from the right to the left atrium.
This is one way blood bypasses the fetal lungs.Second, blood flowing from the right ventricle into the pulmonary trunk bypasses the pulmonary arteries through the ductus arteriosus, which connects the pulmonary trunk and the aorta. In the fetus, the pressures in the right side of the heart are greater than those of the left side, since relatively little blood is returning from the lungs to the left side. As a result, the pressure is higher in the pulmonary trunk than the aorta, and blood therefore passes across the ductus arteriosus from the trunk to the aorta, bypassing the pulmonary circulation.
At birth, when the neonate takes its first breath and inflates its lungs, the resistance in the pulmonary capillary bed falls precipitously. The increase in oxygenation of the newborn’s blood constricts the ductus arteriosus. Within a few minutes, this formerly large vessel has shrunk drastically. Within the first week of life, it closes completely, becoming a fibrous band, the ligamentum arteriosum, identifiable grossly between the pulmonary trunk and the aorta.
These changes abruptly increase blood flow to the now low-resistance pulmonary capillary
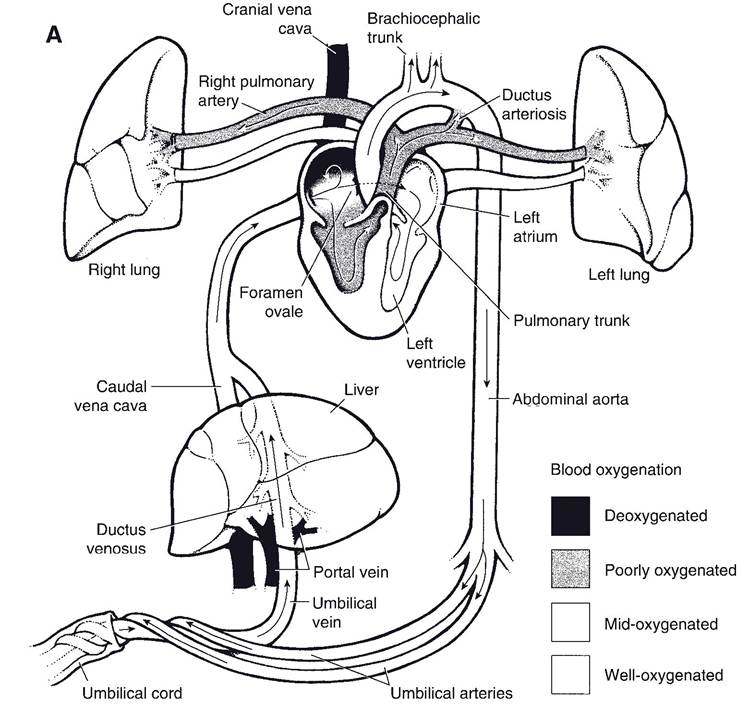
Figure 17-10. Transition between fetal (A) and adult (B) circulation. Fetal modifications include the foramen ovale, ductus arteriosus, umbilical vessels, and the ductus venosus. After birth, the ductus arteriosus and ductus venosus collapse and become ligamentous, the foramen ovale closes, and the umbilical vessels become round ligaments. (Reprinted with permission of Wiley-Blackwell from Smith B.J. Canine Anatomy. Baltimore: Lippincott Williams & Wilkins, 1999.) (Continued)
beds. This abrupt increase in flow to the lungs produces a dramatic increase in blood returning to the left atrium, and as a consequence, pressures in the left side of the heart increase markedly. Greater blood pressure in the left atrium squeezes shut the foramen ovale, and blood no longer flows between the two atria.
A ductus arteriosus that fails to close is a patent ductus arteriosus (PDA). In PDA, the conduit between the low-pressure pulmonary trunk and the high-pressure aorta persists, and blood passes from the aorta into the pulmonary circulation. This overperfuses the pulmonary capillary beds and increases the amount of blood returning to the left atrium, which dilates (is stretched). The left A-V valve is often affected by left atrial dilation in such a way as to allow regurgitation of blood. The overdistension of the left atrium is compounded, and pulmonary congestion may result.
Other modifications of circulation outside of the heart and great vessels take place at birth. one of the most obvious changes is that the
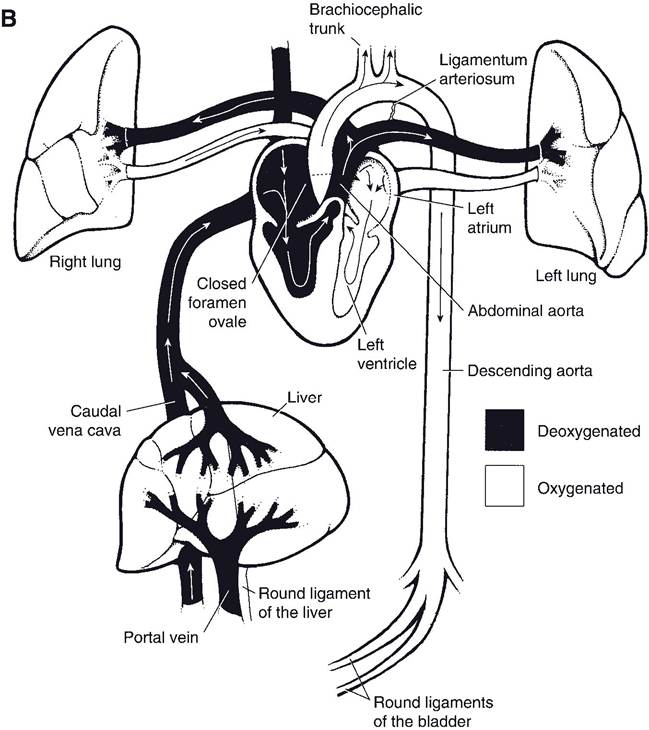
Figure 17-10. Continued
placenta loses its role as oxygenator and provider of nutrients. The vasculature associated with it (umbilical arteries and veins) collapses and converts into fibrous cords (round ligaments) that are sometimes identifiable grossly in the adult. The ductus venosus undergoes constriction as well. If the ductus venosus fails to close completely, blood returning from the viscera via the portal vein may find its way back to the systemic circulation (specifically, the caudal vena cava) without first being processed in the liver. This abnormality constitutes a portosystemic shunt (sometimes called portocaval shunt) and can produce abnormalities of metabolism, growth, and neural function.