FUNCTIONAL ANATOMY
An indication of the exacting task required of the heart is provided by the following figures, culled from various sources: 60% of the total volume of blood within the human body passes through the heart each minute, and the corresponding figures for dogs and horses are 80% and 100%, respectively.
Coordinated contraction is essential for efficient pumping; asynchronous contraction of muscle fascicles (fibrillation) is ineffectual and is rapidly fatal when it involves the ventricular muscle. The sinuatrial node is the pacemaker from which the wave of excitation normally spreads to all parts of the muscle; it has the highest rate of spontaneous activity when relieved from external stimuli, but in normal circumstances its discharge is determined by the fine balance of accelerating sympathetic and retarding vagal inputs. The wave of excitation that spreads from the sinuatrial node through the atrial muscle soon reaches the atrioventricular node (Figure 7-14/2 and Figure 7-16, A-B). This does not respond at once, and the short delay permits completion of atrial contraction. The impulse then spreads to the ventricular muscle through the atrioventricular conducting tissue. Although ventricular contraction is almost synchronous, the subendocardial layer, which includes the papillary muscles, gains a slight lead.
The flow of blood is related to these activities. Blood enters the atria for as long as the pressure within the veins exceeds that within the heart. Several factors of uncertain and varying magnitude contribute to the venous pressure. The force exerted upstream (vis a tergo) is the summation of the following: the residual pressure imparted to the blood by ventricular contraction; the forces exerted by muscles, visceral activity, and arterial pulsation; and the contraction of the diaphragm (the so-called abdominal pump) expelling blood from the caudal vena cava and its large tributaries within the abdomen.
The downstream force (vis a fronte) oscillates between a negative aspirating effect (provided by thoracic expansion and atrial relaxation) and a positive pressure developed on atrial systole. A lateral pressure may be exerted by contraction of the muscular coat of the great veins. Gravity also plays a part, sometimes assisting and sometimes impeding flow according to posture. Much blood flows directly into the ventricles through open atrioventricular ostia, and only a “topping-up” effect is exerted by the atrial contraction, which coincides with the last stage of ventricular relaxation. When the atria do contract, some blood may reflux into veins (despite the conjectured throttle mechanism already mentioned); a jugular pulse may be visible evidence of this, most seen in cattle.The pulmonary and aortic (arterial) valves are closed during ventricular relaxation when the arterial pressure exceeds that within these chambers. Ventricular contraction closes the atrioventricular valves; eversion of the cusps into the atria is prevented by the timely contraction of the papillary muscles. As the contraction develops, blood forces the arterial valves open and the conducting arteries are expanded by this sudden input. The two ventricles do not contract identically. The right ventricular lumen is squeezed in a bellows action in which the outer wall is drawn toward the septum (Figure 7-23). The more cylindrical left ventricle contracts radially and in length; radial contraction is believed to have the greater effect.
Closure of the heart valves produces distinctive sounds that are audible on auscultation. Their character provides valuable information on the condition of the
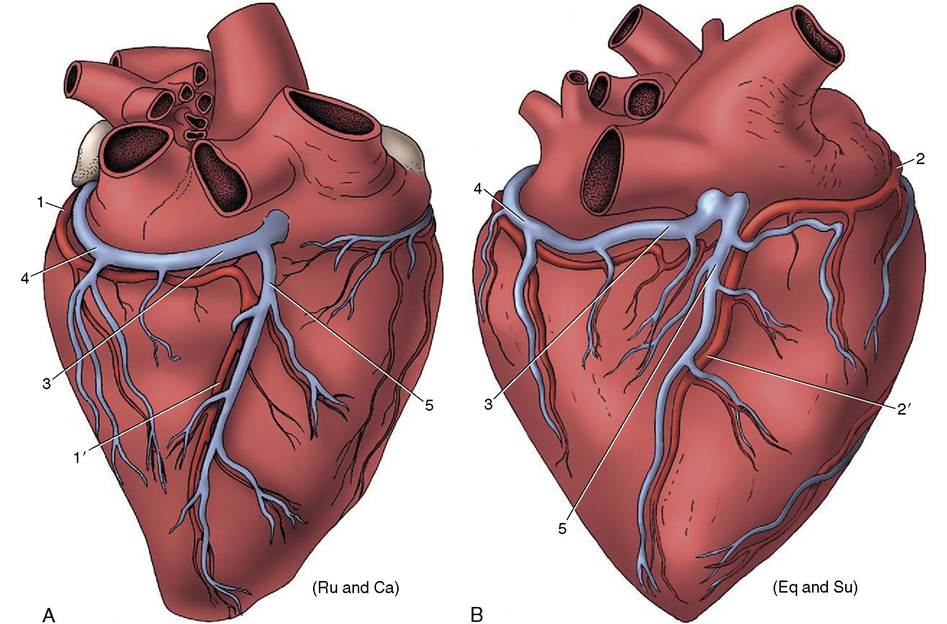
Figure 7-19 Patterns of coronary circulation of the heart viewed from the right. A, Situation in ruminants and carnivores; the right (subsinuosal) interventricular branch (T) is a continuation of the left coronary artery.
B, Situation in the horse and pig; the right (subsinuosal) interventricular branch (2') is a continuation of the right coronary artery. Ru (ruminants), Ca (cat), Su (pig), Eq (horse). 1, Circumflex branch of left coronary artery; 1', right (subsinuosal) interventricular branch; 2, right coronary artery; 2', right (subsinuosal) interventricular branch; 3, coronary sinus; 4, great cardiac vein; 5, middle cardiac vein.valves. Because of the vagaries of sound conduction through tissues of different densities, the projections of the heart valves on the chest wall are not necessarily the spots (puncta maxima) where the sounds are most clearly heard. As a rough guide, if species and breed variations and other factors are not considered, it may be said that the pulmonary, aortic, and left atrioventricular valves are best auscultated over the third, fourth, and fifth ribs of the left side, and the right atrioventricular valve is best auscultated over the fourth rib on the right. The arterial valves are somewhat dorsal to the atrioventricular valves, although the slope of the heart is clearly relevant to this detail. Percussion is also used as a means of evaluating the size of the heart. The quality of cardiac dullness contrasts with the high pitch obtained when percussion is performed over the lungs. The boundary of the cardiac area is not sharply defined because the lung tissue covering the heart grades in thickness about the cardiac notch.