Functional road map of the nervous system
Using a map of the nervous system that depicts the main pathways and functional areas, the clinician can determine what signs the animal will have with lesions in different regions.
Conversely, given a set of clinical signs, the clinician will be able to use the map to identify where the lesion is likely to be.The following is a summary of the location of the functions that are assessed in a neurological examination. From this NeuroMaps of the brain and spinal cord have been drawn (Figs. 13.14 and 13.15).
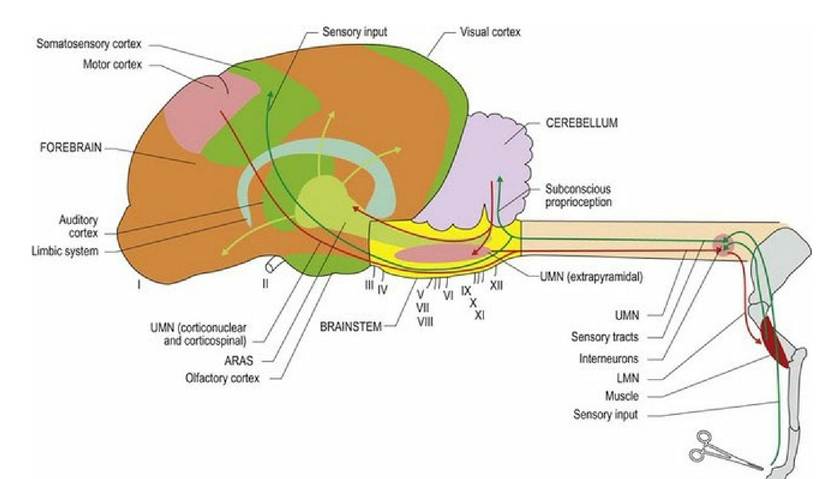
Fig. 13.14 NeuroMap depicting main neural functions assessed in a neurological examination. If a focal area of the map is covered representing a lesion, then it can be seen which neural functions would be compromised and which would not be affected. The brain is divided into three functional regions - forebrain (orange), brainstem (yellow) and cerebellum (purple) (see also Fig. 4.11 for main functional regions of the brain). Green lines indicate sensory systems and red lines identify motor systems. ARAS = ascending reticular activating system; UMN = upper motor neuron, LMN = lower motor neuron.
Anatomical basis of the neurological examination: key points (see specific chapters for details)
Proprioception (Chapters 4, 6, 7, 8)
(a) The pathways for subconscious proprioception are as follows.
From the body and limbs: muscles and tendon receptors, spinal nerves, dorsal horn of spinal cord, ipsilateral lateral funiculus (mostly), brain stem, ipsilateral cerebellum.
From the head: Vestibular receptors of the inner ear, vestibular portion of CN VIII, vestibular nuclei of brainstem, cerebellar peduncles (caudal), ipsilateral cerebellum.
(b) The pathways for conscious proprioception are as follows:
From the body and limbs: tactile receptors and muscle spindles, spinal nerves, dorsal horn, ipsilateral dorsal and lateral funiculus, brain stem, decussates, thalamus, contralateral somatosensory cortex.
From the head: Vestibular receptors of the inner ear, vestibular portion of CN VIII, vestibular nuclei of brainstem, decussates in brainstem, thalamus, contralateral somatosensory cortex.
Motor fUnction (Chapters 4, 5, 7, 8, 9)
Motor planning centres are located in the forebrain, whereas motor coordination occurs in the cerebellum.
Upper (central) motor neuron centres are located in the motor cortex and the brainstem. UMN tracts connect locally to LMN in cranial nerve nuclei of the brainstem. UMN tracts also travel caudally along the spinal cord to influence LMNs. UMNs in the lateral funiculi, facilitate flexor muscle activity; UMNs in the ventral funiculi facilitate extensor muscle activity.
Lower (peripheral) motor neurons arise in the CNS, but their axons leave it via cranial and spinal nerves and connect with muscles (somatic or visceral) at neuromuscular junctions.
For reflex activity, sensory fibres from peripheral receptors connect with LMNs of cranial nerves, or LMNs of spinal nerves in the brainstem or spinal cord, respectively.
Behaviour and memory (Chapter 11)
These functions are associated primarily with the forebrain limbic system (e.g. hippocampus and associated structures).
Arousal (Chapter 11)
Mental awareness is associated with the ascending reticular activating system (ARAS) of the brainstem and diffuse areas of the forebrain. Mental awareness can be decreased with relatively focal lesions in the ARAS of the brainstem or with diffuse lesions affecting widespread areas of the forebrain. Examples of focal versus diffuse lesions would include a tumour in the brainstem or hepatic encephalopathy, which globally affects the forebrain.
Cranial nerves (Chapter 10)
The anatomical basis for cranial nerve function is covered in Table 13.2.
Nociception (Chapter 6)
F or withdrawal reflex fUnction
For the limbs: Nociceptor, spinal nerves, dorsal horn, ventral horns of multiple spinal cord segments in that intumescence, LMNs to flexor muscles of that limb causing flexion of the limb.
Additionally, in the standing animal, the other limbs, especially the contralateral one will be reflexively stimulated to extend, to carry additional weight.From the head: nociceptor, primarily the trigeminal nerve, CN V (also CNN VII, IX and X from the oral cavity and external ear), to the spinal nucleus of CN V (medulla oblongata). Reflex connections occur with the motor nucleus of the facial nerve for facial muscle contraction, nuclei of CNN III, IV and VI for eyeball movement and IX and X (nucleus ambiguus) for gagging.
For conscious perception
From the body and limbs: nociceptor, spinal nerves, dorsal horn, dorsal funiculus (for Aδ-fibre input), lateral and ventral funiculi (for C-fibre input). C-fibre nociception is projected cranially in multiple pathways, some of which are bilaterally represented and may have multiple synapses. Tracts and pathways decussate in the brainstem, travel to the thalamus and the contralateral somatosensory cortex.
From the head: nociceptor, trigeminal nerve (CN V), spinal tract of V in the medulla oblongata, fibres decussate and travel rostrally (trigeminal lemniscus), to the thalamus and to the contralateral somatosensory cortex.
Spinal pain
The anatomical basis involves sensory receptors in muscles, ligaments, tendon, periosteum and meninges; sensory spinal nerves, especially the C-type fibres, input into the associated spinal cord region and transmission as for nociception to the contralateral somatosensory cortex.