The NeuroMap: Overview of the nervous system
The NeuroMaps are functional road maps of the neuraxis (Figs. 13.14 and 13.15). They depict the location of the neural functions that are evaluated in the neurological examination.
The NeuroMap allows the clinician to see which functions would be compromised, AND which functions would still be normal, if there was a lesion in a particular area. For example, a lesion in the spinal cord could compromise both conscious and subconscious proprioceptive pathways and UMN pathways, causing gait deficits. However there are no cranial nerves or centres associated with arousal in the cord, so these functions will be normal. The following is a repeat of two key concepts that have been stated previously; these are fundamental to understanding lesion localisation (1) Noting which neural systems are functioning normally is just as important as noting those that are dysfunctional; (2) It does not matter much where the lesion is located on a pathway - origin, midpoint or termination, the clinical signs of dysfunction will be similar. This is analogous to a battery (origin), linked by a wire (midpoint) to a light bulb (termination). The light will only work if the all three components are functioning.Summary of functions in the neuraxis
Table 13.4 has been constructed using the NeuroMap in Fig. 13.14 and can be used in conjunction with it. It tabulates which functions are associated with each region of the brain and the generalised spinal cord. A specific NeuroMap of the spinal cord is given in Figure 13.15 and effects of lesions in different regions are summarised in Table 13.5. From the NeuroMap, it can be predicted which neural functions could be compromised by lesions in the different areas of CNS. For example, reading down the column associated with the forebrain in Table 13.4, it can be seen that a forebrain lesion may cause dysfunction in contralateral conscious proprioception, nociception and vision, but the rest of the cranial nerves and gait will be reasonably normal.
(It is unusual to detect olfactory deficits in forebrain disease.) If the animal has reduced alertness, then the lesion involves extensive areas of the forebrain. Decreased voluntary use of the contralateral side of the body may be observed.Table 13.4 Summary of neural functions that are associated with the different regions of the neuraxis
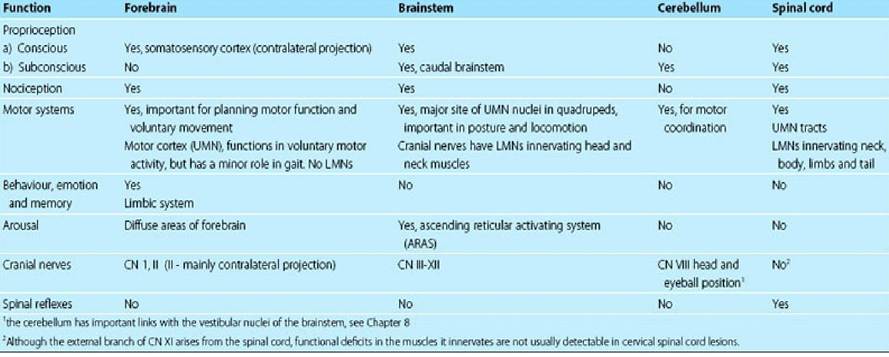
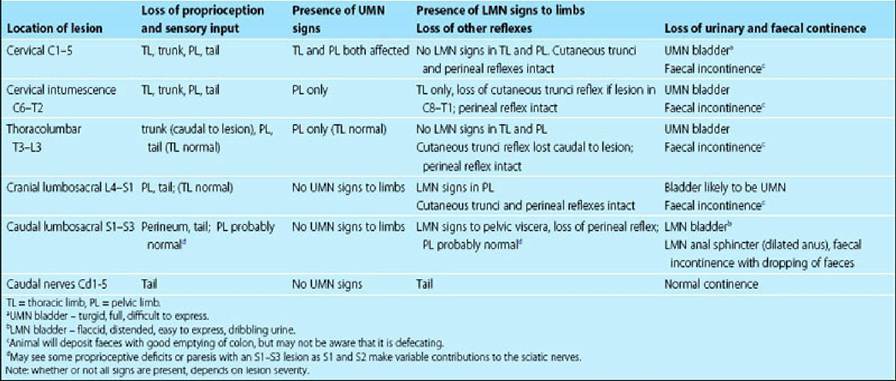
Table 13.5 Summary of effect of lesions in different areas of the spinal cord
Signs of dysfunction in different regions of the neuraxis
Listed in the following text are signs that can occur with lesions affecting different regions of the neuraxis. Note that not all signs may occur depending on the precise location of the lesion and its severity.
Forebrain disease
Abnormal neurological function
■ Conscious proprioception (CP) deficits (knuckling and stumbling) on the contralateral side of the body, but ambulation/gait and posture are still quite good indicating retained subconscious proprioception and motor strength.
■ Could have hypoalgesia (decreased nociception) on the contralateral side, this is more readily detected by testing head nociception.
■ Decreased voluntary motor function of the contralateral side of the body (e.g. kitten playing with a ball).
■ Deficits in vision (contralateral).
■ Deficits in olfaction, although it may be difficult to appreciate reduced olfaction.
■ Reduced arousal if the lesion involves widespread areas of the forebrain.
■ Altered behaviour and emotion and potentially memory (e.g. loss of learned behaviour such as toileting).
Normal neurological function
■ It would not affect CNN III-XII, most of the UMN nuclei, subconscious proprioception, motor coordination, therefore gait will be quite good.
■ Spinal reflexes will be present and spinal hyperpathia will not be present.
Brainstem disease
Abnormal neurological function
■ Conscious proprioceptive deficits (knuckling and stumbling) as pathway is passing through the brainstem to the forebrain.
■ Subconscious proprioceptive deficits (ataxia, base wide/narrow posture) if caudal brainstem disease.
■ Nociception (especially superficial, Aδ-fibre input) could be reduced especially from the head and possibly from the body too, as that pathway passes through the brainstem going to the forebrain.
■ Decreased motor function - there are many UMN nuclei and UMN axons in this area; this would show up as paresis and deficits in gait.
■ Decreased arousal due to effect on ascending reticular activating system.
■ CNN dysfunction that is specific to the rostral brainstem
■ CNN III-VIII dysfunction.
■ CNN dysfunction that is specific to the caudal brainstem
■ CNN IX-XII dysfunction.
Normal neurological function
■ It would not affect CNN I or II (forebrain).
■ Spinal reflexes will be present and spinal hyperpathia will not be present.
Cerebellar disease
Abnormal neurological function
■ Subconscious proprioceptive deficits causing postural deficits affecting limbs, trunk and head, both at rest and during motion; wide- or narrow-based stance; ataxic gait, truncal sway; circumduction or crossing over of feet during ambulation. Delayed protraction of limbs.
■ Tremor due to incoordination of agonist-antagonist muscle function.
■ Hypermetria with increased rate, range and force of movement.
■ Spasticity due to decreased inhibitory effect of cerebellum on brainstem UMN centres.
■ Damage to the VestibulocerebellumZflocculonodular lobe can cause postural disturbances, head tilt and nystagmus.
■ The menace response may be decreased with diffuse cerebellar disease.
Normal neurological function
■ Conscious proprioception should be normal.
■ The animal is not paretic (weak), if anything it tends to spasticity.
■ Most cranial nerves function normally (see comments re CN VIII and menace response).
■ The animal is bright and alert.
■ Spinal reflexes will be present and spinal hyperpathia will not be present.
Spinal cord disease
See Fig. 13.15. The effects of lesions in different regions of the spinal cord are summarised in table 13.5.
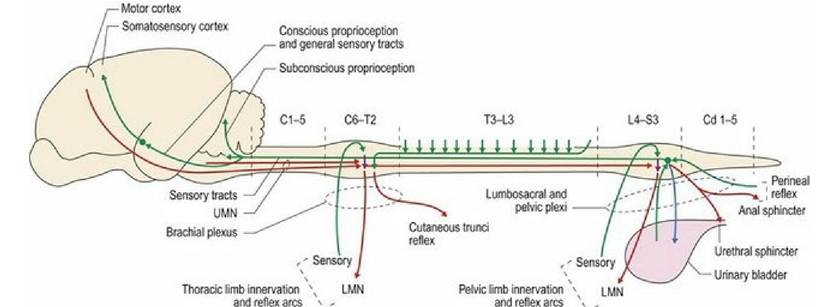
Fig. 13.15 NeuroMap of the spinal cord. Green indicates sensory systems (conveying tactile, thermal, proprioceptive and nociceptive stimuli), red identifies motor systems and blue identifies autonomic systems.
UMN = upper motor neuron, LMN = lower motor neuron
Abnormal neurological function
■ Conscious and subconscious proprioceptive deficits occur as both types of proprioceptive pathways travel cranially through the spinal cord. These deficits result in stumbling, ataxia and dysmetria (altered rate, range and force of movement).
■ Decreased motor function (paresis/paralysis) - due to effects on either UMN tracts or LMNs.
■ Spinal reflexes may be lost if the lesion affects the spinal cord segments associated with that reflex. Exaggerated spinal reflexes may occur with UMN lesions.
■ Hypotonia and atrophy of specific muscles if LMN cell bodies in the spinal cord are damaged.
■ Spinal hyperpathia may be present and can be quite helpful in localising the lesion.
Normal neurological function
■ Behaviour, emotion, memory and arousal would be normal.
■ Cranial nerve function would be normal.
Spinal nerve disease
Abnormal neurological function
■ Loss of afferent (tactile, proprioceptive, nociceptive) input.
■ Paresis, (short steps, the animal appears weak) due to loss of LMN output.
■ Loss of efferent innervation to muscle may result in LMN signs decreased Reflexes, significant muscle Atrophy and decreased muscle Tone (the Neuro RAT - Fig.
5.6).Neuromuscular disease
Neuromuscular disease is caused by lesions of the peripheral motor unit. The motor unit involves the LMN cell body, efferent spinal nerve, neuromuscular junction and muscle. Thus the animal could have LMN signs with hypometria, reduced/absent reflexes. Marked atrophy and loss of tone may be present if the neuromuscular junction is destroyed, but not if it is maintained as in myasthaenia gravis.
In myopathies, the main signs can include stiffness, paresis, reduced reflexes and atrophy. Myalgia and changes in muscle bulk may be present, with muscle swelling or atrophy in acute versus chronic cases, respectively.
It the disease purely involves the LMN, NMJ or muscle, then the animal’s proprioception should be normal, but it may be too paretic to demonstrate this well.
Multifocal disease
In cases of multifocal disease, a single lesion cannot account for all the signs. For example, an animal with visual deficits and a head tilt has to have a lesion in the eyes, optic nerves or visual pathways in the forebrain, and the inner ear or brainstem to involve the vestibular system. Another example would be an animal with tremor and hypermetria (cerebellar) as well as lower motor neuron signs to the pelvic limbs (LMNs arising from L4-S1 spinal cord). The most common cause of multifocal signs in animals is inflammatory disease. Multifocal neoplasia or generalised neuropathies may also cause multifocal signs.