Hands-on testing
With respect to the hands-on neurological testing, every clinician has their own approach, but here is an example of an approach that is generically useful for most animals. More detailed information on the neurological examination of large animals is given in books such as Large Animal Neurology, by Ian G.
Mayhew, Blackwell Publishing, 2009, or Veterinary Neuroanatomy and Clinical Neurology, by deLahunta A and Glass E, 3rd edition, Saunders, 2009.Proprioception and motor function
A key concept to comprehend is that proprioceptive testing also evaluates motor function as the animal has to move the body to perform the test. When evaluating proprioception in a limb, try not to disturb the overall position of the trunk too much as this stimulates proprioceptors throughout the body, rather than just the limb being examined, reducing the specificity of the test.
Hopping
This test is good for evaluating subconscious and conscious proprioception and may be performed, with care, in some large animal patients. In small animals, one leg is held flexed, e.g. the left thoracic limb, and the animal is pushed gently to the right. As the centre of gravity moves laterally over the right thoracic limb, this changes the subconscious proprioceptive input from the muscle spindles (stretching of muscles), joint angle receptors and Golgi tendon organs. It also changes conscious proprioceptive input by stimulating tactile receptors in the feet. In the normal animal, this will induce a lateral hop to replace the limb back under the centre of gravity. In small animals, it is useful to have the animal still bearing weight on the limb girdle that is not being tested. For example, if testing the thoracic limb, let the animal bear weight on its pelvic limbs. Thus the animal pivots in an arc around the supporting limbs; that is around the pelvic limbs when testing the thoracic limbs and vice versa.
This makes testing easier for the clinician as they don’t have to try to lift the animal clear of the floor. Animals hop better laterally then medially, so only hop them laterally. Count the number of hops the animal makes on that leg, then test the other leg of the same girdle, through a similar size arc. Counting the number of hops, helps the clinician identify asymmetry between the limbs. The number of hops to cover a certain distance will depend on the size of the animal; a tall dog like a Labrador retriever takes bigger steps than a little dog like a Dachshund. An increase, or decrease, in the number of hops may indicate reduced motor or sensory function, respectively. Thus, the clinician can try to differentiate reduced proprioception from reduced motor function. An animal that has purely motor deficits resulting in reduced motor strength (e.g. myopathy) may not be able to hop properly, even though it has intact proprioception by which it can sense that its feet are not in a good weight-bearing position. Supporting the animal, by holding one hand underneath it, reduces the motor effort required to move the limb and the animal will move, or attempt to move the limb as soon as it senses abnormal limb position, but being weak, the hops will be shorter. Comparatively, if the animal has a proprioceptive deficit, it will not attempt to move the limb as soon as it is no longer in a good weight-bearing position under the body. The centre of gravity must be shifted further, creating a stronger proprioceptive stimulus to finally induce a hop. Thus the hop, if it occurs, will be bigger.Paw position response (knuckling)
This test is more specific than hopping for evaluating tactile receptors compared with muscle receptors, thus it is good for conscious proprioceptive testing. The animal’s weight is gently pushed to the opposite side, reducing the amount being carried on the leg being tested, then the toes are flipped under (Fig. 13.5). To test for subtle dysfunction, the clinician may just turn under a single toe.
The body weight is redistributed back over the limb being tested and the animal is observed to see if it corrects the foot position. To avoid stimulating joint angle and muscle receptors in the proximal leg, the clinician tries to turn the toes under without lifting the leg.
Fig. 13.5 Paw position response or ‘knuckling’ test. The foot is turned over so the animal to see if the animal will bear weight on the dorsum of the paw (the knuckles).
Reflex stepping - the sliding paper test
The following test is more subjective and requires practice and experience to learn to read its results. It is only suitable for small animals, not horses or farm animals. As the name implies, this test consists of placing the animal’s foot on a piece of paper and sliding the paper laterally. This alters the relationship between that supporting limb and the animal’s centre of gravity. It changes proprioceptive input, especially from the muscle and tendon receptors in the proximal limb (extrinsic muscles), thus it can be good for identifying subconscious proprioceptive deficits. Its principles are similar to hopping. When the limb is no longer in a good weightbearing position, the normal animal should lift the limb and step it back into a weight-bearing position. The replacing of the limb will be delayed or absent in an animal with proprioceptive dysfunction.
Hopping and paw position response (knuckling) are the two most helpful tests. Interpreting the sliding paper test requires experience, but can help to identify deficits in subconscious proprioception. This latter test and hopping both disturb the position of the props (limbs) with respect to the centre of gravity. Thus both tests may be abnormal with lesions affecting subconscious proprioceptive pathways. The paw position response is most likely to be abnormal if the conscious proprioceptive pathways are affected. Thus in a spinal cord lesion, all three tests may be abnormal.
With cerebellar disease, hopping and sliding paper test are likely to be affected, whereas with forebrain lesions, the hopping and paw position response are likely to be affected.In large animals, ‘paw position’ cannot be reliably assessed and hopping tests can be hazardous. Instead time is spent assessing the gait for evidence of dysmetria (decreased or increased joint movement), particularly when visual and vestibular input is altered. For example, the animal is walked down a slope with its head raised. For movements to be performed correctly, conscious and subconscious proprioceptive pathways all have to function normally.
Identifying asymmetry in proprioceptive function
To identify if one side of the body is more severely affected than the other, tests that involve both pelvic limbs or both thoracic limbs are used; this includes the extensor postural thrust test and wheelbarrowing, respectively. For the extensor postural thrust test, the animal is lifted up so that its back feet are dangling. The animal is lowered and when the back feet contact the ground the normal animal will extend/thrust reflexively. However, as the feet contact the ground too far forward to bear weight properly, they will step their feet backwards until the feet are in a weight-bearing position. In an animal with neurological deficits either of proprioception or motor function, that backward stepping can be asymmetrical with reduced stepping on the more affected side. In the wheelbarrowing test, the animal’s back feet are lifted just clear of the ground, and the animal is pushed slowly forward (Fig. 13.6). This will exaggerate any paresis and asymmetry of the thoracic limbs.

Fig. 13.6 Wheelbarrowing in a dog.
There are other tests such as hemiwalking, tactile and visual placing, hip sway that may be helpful to confirm subtle lesions. (For details of tests see either deLahunta or Mayhew, cited on the previous page).
Cranial nerves
The function of most cranial nerves can be assessed by observation, but hands-on testing helps to confirm specific functions.
Testing cranial nerve function is outlined in Table 10.2 (see also Fig. 10.13). Cranial nerve reflexes are described below and the anatomical basis of the these reflexes is given in Table 13.2.Table 13.2 The anatomical components of cranial nerve function
| Test | CNS region involved | CNN being evaluated |
| Palpebral reflex | Brainstem | CN V (a) and VII (e) |
| Upper eyelid near medial canthus | CN V ophthalmic branch | |
| Lower eyelid near lateral canthus | CN V maxillary branch | |
| Auriculopalpebral reflex | Brainstem | CN V (a) (maxillary branch) and VII (e) |
| Facial sensation - tactile stimulation | Brainstem and forebrain | CN V (a) |
| Upper eyelid and nasal mucosa | CN V ophthalmic branch | |
| Ventral eyelid and muzzle | CN V maxillary branch | |
| Skin of the chin | CN V mandibular branch | |
| Masticatory muscle bulk, jaw tone - palpation | Brainstem | CN V (e) mandibular branch |
| Olfaction observe the animal sniffing an object | Forebrain | CN I (a) |
| Menace response - threatening hand movement towards the eye. | Forebrain, brainstem (and cerebellum) | CN II (a), CN VII (e), also CN VI (e) (eyeball retraction) |
| Vestibulo-ocular reflex and eyeball position | Brainstem | CN VIII (a), III, IV, VI (e) |
| Tongue shape and movement | Brainstem | CN XII (e) |
| Gag reflex | Brainstem | CN IX, X (a) and (e) |
| Pupillary light reflex | Forebrain and brainstem | CN II (a), III (e) |
| Dazzle reflex | Forebrain and brainstem | CN II (a), VII (e) |
(a) = afferent, (e) = efferent.
Note that as cranial nerves are bilaterally paired, both sides of the head must be checked.
(a) Pupillary light reflex. Shining a light into the eye (CN II a = afferent) will cause constriction of the ipsilateral pupil and lesser constriction of the contralateral pupil (CN III, parasympathetic, e = efferent). These reflexes are called the direct and indirect PLR, respectively (see Fig. 10.8).
(b) Dazzle reflex. Shining a bright light into the eyes (CN IIa) causes partial narrowing of palpebral fissure (CN VIIe).
(c) Palpebral reflex. Tapping the skin around the eye (CN Va) induces reflex contraction of the orbicularis oculi muscle (CN VII) and closure of the palpebral fissure.
(d) Auriculopalpebral reflex. Lightly stimulating the skin just rostral to the opening of the external ear canal (CN Va) induces contraction of the orbicularis oculi muscle (CN VIIe) and partial closure of the palbebral fissure.
(e) Vestibulo-ocular reflex. Moving the head from side to side, or vertically (CN VIIIa), will induce fast, flicking movements of the eyeballs (CNC III, IV and VIe) in the direction that the head is travelling (Fig. 13.7).
(f) Corneal reflex. This is a noxious and potentially damaging stimulus and only performed if the palpebral reflex is dysfunctional. Gently touching the cornea with a moistened cotton swab (CN Va) causes closure of
the eyelids (CN VIIe).
(g) Gag reflex - Stimulation of the back of tongue and pharynx (CN IX and Xa) with fingers causes gagging with pharyngeal contraction (CN IX and Xe).
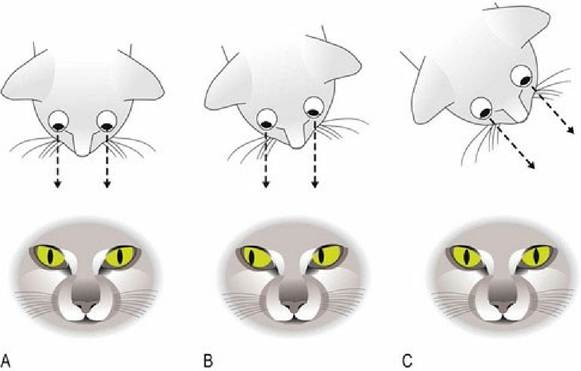
Fig. 13.7 Vestibulo-ocular reflex. As the head moves, the gaze remains fixed on a position (A to B), so the eyes move slowly in the orbits until they suddenly and rapidly flick in the direction that the head is moving and become centred in orbit once more (C).
A note on the menace response: When a threatening gesture is made to the eye in a normal animal, it will blink and/or pull its head away (Fig. 13.8). The gesture should be made from different positions with respect to the eye so that the temporal and nasal field of view are tested. This is not a reflex however. It is a response as it has to be learnt; it is not hard-wired at birth. In precocial animals, such as foals, it develops 710 days after birth whereas in altricial animals such as puppies, it can take up to 4 months. It primarily utilises sensory input via the optic nerve (CN II) and output via the facial nerve (CN VII) to close the palpebral fissure. It may also utilise a tract (tectotegmentospinal tract) from the midbrain to the cervical spinal cord to stimulate neck muscle contraction and head movement. The CNS connections involve the entire brain, including forebrain (reception of input) and brainstem (motor output); the cerebellum is also involved (coordination).

Fig. 13.8 The menace response test being performed in a zebra that had head trauma. The zebra failed to
blink in response to the threatening gesture indicating dysfunction in either CN II, the central connections in the brain, or CN VII.
The ocular fundus should also be examined as retinal and optic disc lesions may arise in some neurological conditions.
Muscle bulk and tone
After completing the examination of the cranial nerves, the clinician runs their hands over the head, neck, trunk and limbs checking muscle bulk. The small animal is laid on its side to evaluate the limbs more closely. Each limb is flexed and extended to test for resistance to movement, which indicates muscle tone. The bulk of specific muscles may be rechecked if necessary and then the spinal reflexes are assessed. Reduced or no Tone, and marked muscle Atrophy are two of the three characteristic signs of LMN disease (remember the Neuro RAT see Fig. 5.6).
Spinal nerve reflexes
Clinically, the reflexes are tested to evaluate the integrity of the different components of the reflex arc (see Fig. 4.3). Disruption of sensory input, CNS interconnections, or LMN output will result in decreased, or loss of, reflex activity. This is most commonly seen with LMN lesions involving the region of the CNS in which the LMN cell body is housed, or in the LMN itself. A decrease in, or loss of, the reflex is highly localising as it indicates precisely which parts of the PNS and CNS must be compromised (Table 13.3). If the reflex arc is present then the three anatomical components are intact and functioning.
Table 13.3 The anatomical components of spinal reflexes
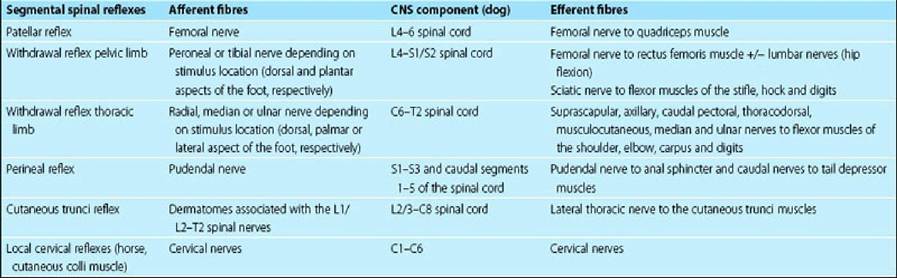
Clinically, an intact reflex, be it normal or exaggerated, tells the clinician that the lesion does not involve that area of the CNS or the PNS. It will be present even if the neuraxis cranial or caudal to the reflex circuit has been severed. Exaggeration of spinal reflexes may occur with lesions affecting UMNs cranial to the reflex; this is because the UMN system has an overall inhibiting influence on LMN. A UMN lesion in the thoracolumbar spinal cord will compromise UMNs supplying LMNs in the lumbar intumescence. The patellar reflex may be exaggerated or exhibit clonus in which there is sustained stifle extension with tremor; this is more likely with chronic lesions. Note that increased extension of the stifle during patellar reflex testing can also happen when there is loss of tone in the opposing, hamstring muscles due to LMN disease affecting the sciatic nerve; this is called pseudohyperreflexia.
In affected horses that are still ambulatory, it is technically difficult to assess spinal reflexes or motor tone. Signs of UMN dysfunction can be assessed by looking for evidence indicating lack of UMN initiation of voluntary movement, for example, the ability of a horse to resist being pulled to one side by its tail while it is walking (see Fig. 5.7).
Clinically, there are a number of reflexes that can be evaluated in the animal. They include limb and trunk reflexes involving spinal nerves, and head reflexes involving cranial nerves. The anatomical basis of these reflexes is described in Tables 10.2 and 13.3.
The spinal reflexes that can be routinely and reliably tested in companion animals include the withdrawal reflex in the pelvic and thoracic limbs and the patellar reflex in the pelvic limb. These are tested in the recumbent animal. The cutaneous and perineal reflexes can be tested either in the recumbent or standing animal.
Pelvic limb
(a) Patellar reflex. The patellar ligament extends ventrally from the distal aspect of the patella to the tibial crest. It is the continuation of the quadriceps tendon distal to the patella. With the animal in lateral recumbency, the patellar ligament is tapped with a plexor (hammer). This causes abrupt extension of the quadriceps muscle, eliciting its reflex contraction and extension of the stifle joint. If the animal is tense then the uppermost leg may be too extended to permit the reflex. This upper leg tension may be due to the animal lifting its head to that side, preparing to get up. Head turning will stimulate the vestibular system causing ipsilateral extension, overriding the patellar reflex. In that case, it is useful to test the reflex on the downside leg, as that leg will usually be more relaxed (Figs. 13.9 and 5.1).
(b) Withdrawal (flexor or pedal) reflex. Pinching the toes causes flexion of the limb using all the limb flexor muscles innervated by the sciatic nerve and the femoral nerve innervating the rectus femoris muscle of the quadriceps. Hip flexion may also involve the iliopsoas muscle innervated by lumbar nerves. For the withdrawal reflex observe how well the animal can flex each joint in the limb. For example, the hock may not flex well if the animal has a subtle LMN lesion affecting the sciatic nerve (Fig. 13.10).
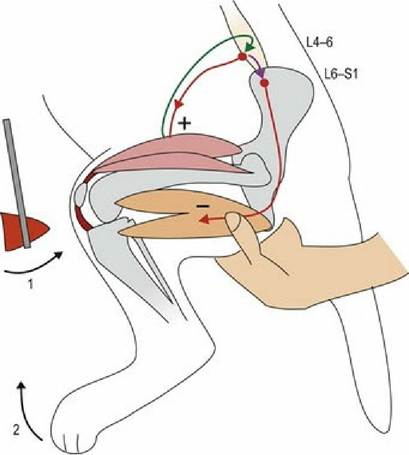
Fig. 13.9 Testing the patellar reflex in the dog. Tapping the patellar ligament with the plexor (1) results in stifle extension (2) (see section on myotatic reflexes).

Fig. 13.10 Testing the pedal/withdrawal reflex in a dog. Barney is reflexively pulling his foot away and showing conscious awareness of the noxious stimulus.
In ambulant horses the patellar reflexes and withdrawal reflexes cannot be assessed.
Trunk
(a) Perineal reflex. Tactile stimulation of the perineal region will cause reflex contraction of the anal sphincter and flexion of the tail.
(b) Cutaneous trunci reflex. This reflex is elicited by pinching of the dorsal skin, 2-3 cm lateral to the spinal column, beginning at the iliac crest and moving cranially to the cranial thorax. In the normal animal stimulation of the truncal dermatomes on one side results in twitching of the skin on the lateral aspect of the thorax bilaterally (Fig. 13.11). In horses and cattle the reflex is best elicited by firmly tapping the skin over the trunk with a blunt instrument such as a pair of forceps.
(c) Neck skin reflexes. In horses, pinching/tapping the skin on the lateral aspect of the neck stimulates contraction of the cutaneous colli muscle. This is a local reflex testing the function of cervical nerves (sensory and motor) and the cervical spinal cord.
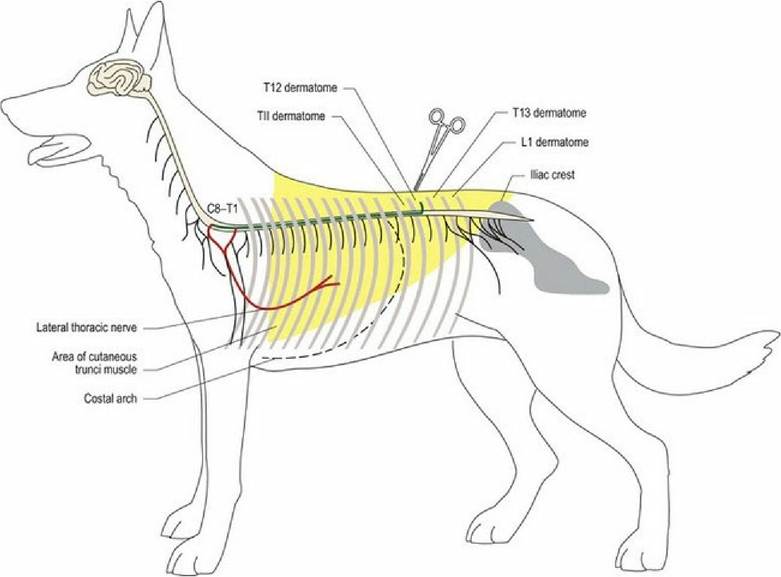
Fig. 13.11 The cutaneous trunci reflex assesses sensation in dermatomes associated with spinal nerves located from the cranial thoracic region to L1 or L2.
Thoracic limb
The withdrawal reflex is the main reflex tested in the thoracic limb and is done by pinching the toes. Withdrawal (limb flexion) involves flexor muscles throughout the limb; these muscles are innervated by a variety of nerves from the brachial plexus.
Nociception
Of clinical importance during the neurological examination is assessing both the reflex action and conscious response of the animal to nociceptive stimuli. The integrity of both the Aδ- (fast- conducting, pin-prick pain) and C-fibres (slow-conducting, acute pain fibres) is evaluated. Both types of fibre synapse in the dorsal horn where they make connections with LMN for a variety of reflex functions, including the withdrawal, cutaneous trunci or perineal reflexes. Input is also transmitted to the brain for conscious perception. Aδ-fibres transmit stimuli from superficial regions (skin) and so can be localised precisely by the forebrain. They travel cranially, primarily in the dorsal funiculus of the spinal cord (fasciculus gracilis and cuneatus). C-fibres are tested using pressure stimuli such as the application of haemostats to the digit. C fibres also convey stimuli from deeply located tissues, e.g viscera, and that may only be poorly localised by the forebrain. These stimuli travel cranially, in lateral and ventral funiculi on both sides of the spinal cord, in a number of different tracts. Both systems pass through the brainstem to synapse in the thalamus and are projected to the somatosensory cortex.
Prognostically, in cases of paralysis, it is essential to determine whether the spinal cord is functionally intact. The last neural function to be lost with increasing severity of spinal cord lesions is nociception from deeply located tissues such as bone. Conveying such nociceptive stimuli are C-type fibres in the PNS and several spinal cord tracts sited in different funiculi. To evaluate whether an animal perceives a noxious stimulus requires that a conscious response to the stimulus be observed. A noxious stimulus is applied to the foot by pinching the digit. This stimulus should produce two effects in the normal animal: (a) reflex withdrawal of the foot and (b) conscious perception of the stimulus indicated by the animal turning and looking at the foot, or whining, or pupil dilation due to a response of the sympathetic nervous system (see Fig. 10.10). If the animal only demonstrates the withdrawal reflex but no conscious perception of the noxious stimulus, then the clinician knows that the reflex wiring is intact but the animal probably has a functional, or structural, transection of the spinal cord cranial to the region involved with the withdrawal reflex arc. Thus loss of conscious response to a noxious stimulus usually indicates a guarded or poor prognosis for return of spinal cord function; the outcome for the animal depends on the cause of the lesion and available treatment. Of course, if the LMNs of the withdrawal reflex arc are damaged the withdrawal may be reduced or absent. If the animal shows a conscious response, then that tells the clinician that the spinal cord is not transected (functionally or anatomically). This indicates a better prognosis than if there is no conscious response.
To test nociception in the head, the clinician may stimulate just inside the nares, for example, with the tip of haemostats. This stimulus should result in the animal pulling its head away abruptly. Animals with lesions in the somatosensory cortex may have hypoalgesia and not pull the head away when the nostril contralateral to the lesion is stimulated as the pathway to the somatosensory cortex decussates (Fig. 13.12).

Fig. 13.12 Testing nociception in the head. The vestibule of the external nares is innervated by the ophthalmic branch of the trigeminal nerve; the nasal planum by the maxillary branch of CN V.
Spinal hyperpathia
Hyperpathia refers to increased sensitivity, such that a non-noxious stimulus is perceived as a noxious one. Spinal hyperpathia indicates disease in the vertebral column. It may be focal, as occurs with an extruded intervertebral disc, or extensive as occurs in meningitis. The lesion may be in the vertebrae, intervertebral discs, spinal ligaments, or meninges. The presence of spinal hyperpathia is assessed by palpation and application of focal pressure to the vertebral column. Spinal manipulation, primarily of the neck or lumbosacral region, may also be performed if appropriate. Do not manipulate, or palpate firmly, the vertebral column in any cases in which spinal instability is suspected, for example in cases of suspected trauma or atlanto-axial subluxation. Neck manipulation in cases of caudal cervical malformation-malarticulation (Wobbler) syndrome may exacerbate compression of the spinal cord. Bending the neck may cause redundant ligament to buckle, increasing spinal cord compression. Firm palpation is also not appropriate in spinal trauma cases as structures may be unstable. Palpation is useful for determining sites of intervertebral disc extrusion, but manipulation is not appropriate as it may exacerbate the extrusion.
To assess for areas of sensitivity along the vertebral column, it is useful to have the animal standing (if it can); it can also be done in the recumbent animal. Placing one hand under the abdomen not only supports the animal, but also can detect tensing of the abdominal muscles. In a more stoic animal, that tensing may help indicate when an area of increased sensitivity is palpated.
When palpating the vertebral column, the clinician applies firm pressure to the top or sides of the vertebrae. In the normal animal, this pressure is non-noxious. If the animal has increased sensitivity in the vertebral column already due to a lesion, then that pressure is perceived as noxious and the animal will indicate that behaviourally by tensing, flinching, whining, snapping, or pulling away.
Beginning at the lumbosacral area and moving cranially to T1, the clinician places their fingers and thumb on opposite sides of the spinal column and applies downwards pressure to the transverse processes or heads of the ribs (Fig. 13.13). Having done that, it is useful to start caudally again and apply downwards pressure between each dorsal spinous process. The first run is a general survey of the vertebral column, while the second is more specific, testing for precise areas of pain.

Fig. 13.13 Testing for increased sensitivity by applying downwards pressure along the vertebral column. Note the supporting hand under the abdomen (see text).
For the neck, if no instability is suspected, the animal’s head is gently turned laterally to either side, then dorsally and ventrally. The normal animal should be able to look around at its tail, more than 180° upwards and the nose should be able to point ventrally and caudally between its thoracic limbs. For more precise localisation of hyperpathia, a hand is placed on either side of the neck and pressure applied to the cervical vertebral column from caudal to cranial. Gentle rotational pressure can be applied to the wings of the atlas. Note that the caudal cervical vertebrae are closer to the ventral aspect of the neck than the dorsal. The dorsal aspect of the neck is primarily muscle and nuchal ligament.
Assessing autonomic function
The urinary bladder is palpated for size and tone and, in the incontinent animal, for ease of manual expression. If the animal is incontinent a full, turgid bladder that is difficult to express suggests the presence of an UMN lesion, whereas one that is large, with a flaccid wall and that is easy to express, indicates a LMN lesion involving the urinary bladder (see Fig. 12.8).
In cases of faecal incontinence, the presence or absence of anal tone and the perineal reflex is important in differentiating UMN lesions cranial to the sacral spinal cord from LMN lesions involving the sacral spinal cord or its outflow.
The integrity of the ANS can also be evaluated by assessing pupil size and response to stimulation by light. The amount of ocular, nasal and oral secretions can be assessed, while warmth and colour of the ears can indicate changes in vascular tone. In horses, changes in cutaneous blood flow may result in sweating (see Fig. 12.6). In animals with dysautonomia, there may also be changes in cardiovascular and gastrointestinal function with altered heart rates and gut motility.