Heart Failure Is Compensated for by Both Starling's Mechanism and the Arterial Baroreflex
There are many types and causes of heart failure. Some clinicians use the term very broadly to refer to any condition in which a problem in the heart limits its ability to deliver a normal cardiac output to the body tissues.
Such conditions would include various valve defects, arrhythmias, and even heartworm infestation. A more restrictive definition, and one favored by physiologists, is that heart failure is any condition in which a depressed cardiac contractility limits the ability of the heart to deliver a normal cardiac output. The broad definition of heart failure encompasses virtually any problem with the heart as a pump; a common synonym is pump failure. The more restrictive definition, as used in this chapter, equates heart failure with myocardial failure, a depressed contractility of the heart muscle itself.A depressed cardiac contractility can result from coronary artery disease, cardiac hypoxia, myocarditis, toxins, drug effects, or electrolyte imbalances. If the decrease in contractility affects both sides of the heart, the condition is called bilateral heart failure. In other circumstances, failure may be restricted primarily to either the left ventricle or the right ventricle and thus is called left-sided heart failure or right-sided heart failure.
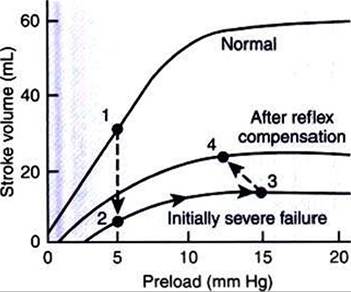
FIGURE 26-1 ■ Ventricular function curves depicting the consequences and compensations for heart failure in terms of changes in preload (end-diastolic ventricular pressure) and stroke volume. See text for details.
Ventricular function curves provide a helpful way to envision the consequences of heart failure and the compensations for heart failure. In Figure 26-1 the curve labeled Normal indicates the relationship between stroke volume and preload for a normal ventricle (for a review» see Figure 21 -3» C).
The curve labeled Initially severe failure shows that a ventricle in failure has a depressed contractility (i.e., a smaller stroke volume for any given preload). If a normal heart suddenly goes into severe failure, stroke volume changes from its normal value (shown by point /) to the low value (shown by point 2). For purposes of illustration, imagine that these curves define the function of the left ventricle and that the left ventricle is the one that fails. A decrease in left ventricular stroke volume causes a decrease in left ventricular output, which results in a decrease in mean arterial blood pressure. If there is inadequate compensation for this fall in blood pressure, severe exercise intolerance is certain, inadequate perfusion of the critical organs is likely, and death is probable. However, several mechanisms react rapidly, within seconds to minutes, to compensate for heart failure and to minimize its adverse effects.One compensation for heart failure is Starlings mechanism. If the left ventricle suddenly decreases its stroke volume, blood dams up (accumulates) in the left atrium and pulmonary veins because the right ventricle, at least for a few heartbeats, maintains a higher stroke volume than the failing left ventricle. Some of the excess blood pumped by the right ventricle accumulates in the left atrium, so left atrial pressure increases. The increase in left atrial pressure creates an increase in left ventricular preload, which leads to an increase in left ventricular end-diastolic volume and (by Starling’s mechanism) an increase in stroke volume. In other words, instead of remaining at the point on the graph labeled 2 (Figure 26-1), the function of the left ventricle moves to the right along the curve of initially severe failure, to point 3, with a higher preload and a somewhat higher stroke volume. This sequence of events, whereby an increase in preload helps offset the fall in stroke volume, is also diagrammed in Figure 26-2 (top left loop).
Note that this compensation does not return stroke volume to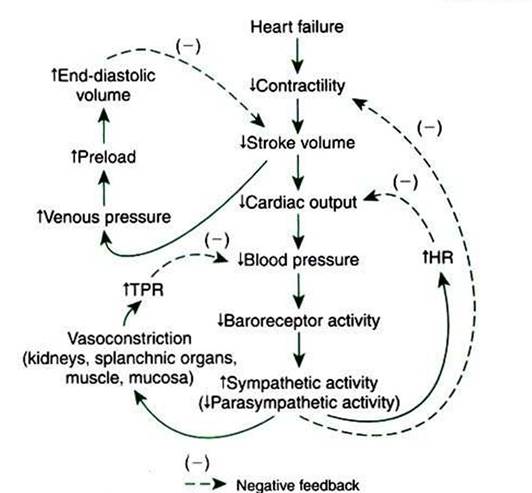
FIGURE 26-2 Consequences and compensations for heart failure.The changes described here include those presented graphically in Figure 26-1. See text for details. HR, Heart rate; TPR, total peripheral resistance.
its normal value, but does bring it to a level somewhat higher than before the compensation.
The arterial baroreflex is another mechanism that reacts rapidly to compensate for heart failure. Because stroke volume remains below normal, even after compensation by Starlings mechanism, left ventricular output also remains below normal, as does arterial blood pressure. Therefore, baroreceptor activity is below normal. The central nervous system (CNS) responds reflexively by increasing sympathetic efferent activity to the heart and blood vessels and by decreasing parasympathetic activity to the heart.
The sympathetic effect on the heart increases ventricular contractility. Contractility is not restored to normal but is brought to a higher level than existed in the absence of reflex compensation. Graphically, the effect of the baroreflex is to move the failing ventricle to a function curve that is intermediate between the “normal'’ curve and the curve of “initially severe failure" (see point 4 in Figure 26-1). Note that the increase in contractility also brings stroke volume back toward (but not reaching) its normal level.
Sympathetic actions on the heart increase heart rate above normal and decrease the systolic duration; these changes also help to restore cardiac output back toward normal despite the persistently depressed stroke volume. Finally, sympathetic activation causes vasoconstriction, particularly in the “non- CriticaT organs, which increases total peripheral resistance (TPR) above normal. This also helps to return blood pressure toward its normal level.
The net effect of the compensations by way of Starling's mechanism and the baroreflex is that blood pressure can be maintained near its normal level, at least when the animal is at rest, despite a severe ventricular failure. Figure 26-2 summarizes these reflex effects. Note that after compensation by Starlings mechanism and the baroreflex, contractility, stroke volume, cardiac output, and blood pressure remain at least somewhat below normal. By contrast, preload, sympathetic activity, heart rate, and TPR are above normal.