Serious Complications Secondary to Heart Failure Include Exercise Intolerance, Edema, Salt and Water Retention, Uremia, Kidney Failure, Septic Shock, and Decompensation
Even though Starlings mechanism and the baroreflex can compensate to a remarkable degree for severe heart failure, important secondary complications often develop. These complications make heart failure a serious clinical problem, even in cases where compensatory mechanisms can maintain cardiac output and arterial pressure at near-normal levels when the animal is at rest.
The first complication secondary to heart failure is exercise intolerance. In a normal animal the ability of the heart to increase cardiac output during exercise depends on sympathetically mediated increases in stroke volume and heart rate. In a patient with heart failure, however, the ability of sympathetic activation to increase cardiac output is almost exhausted simply to restore cardiac output toward normal in the resting state. Therefore the patient’s attempt to exercise is not accompanied by an effective, further increase in sympathetic activity or cardiac output. The failing heart cannot provide the increased cardiac output required to meet the blood flow requirements of exercising skeletal muscle. In the absence of an adequate increase in cardiac output, metabolic vasodilation in the exercising muscle results in a large decrease in arterial pressure and inadequate blood flow to all organs, including the exercising muscle. The patient exhibits lethargy and weakness; even mild exercise leads quickly to exhaustion.
Edetna is another serious complication secondary to heart failure. As noted, blood dams up in the atrium and veins behind a failing ventricle. In the case of left ventricular failure, left atrial pressure increases, as does pressure in the pulmonary veins and pulmonary capillaries. The increase in pulmonary capillary hydrostatic pressure leads to an increase in the filtration of capillary fluid into the interstitial spaces of the lungs. Pulmonary edema develops.
These events are summarized in Figure 26-3 (top left). Excess interstitial fluid in the lungs slows the transfer of oxygen from the lung alveoli into the lung capillaries and can result in systemic hypoxia. In extreme cases, interstitial fluid leaks into the intrapleural space (pleural effusion) or in the alveolar air spaces, which causes a further reduction in lung function. The resulting systemic hypoxia can be fatal. In a patient with right ventricular failure the increase in venous pressure occurs in the systemic circulation. Therefore the resulting edema occurs in the systemic organs, particularly in dependent extremities and in the abdomen.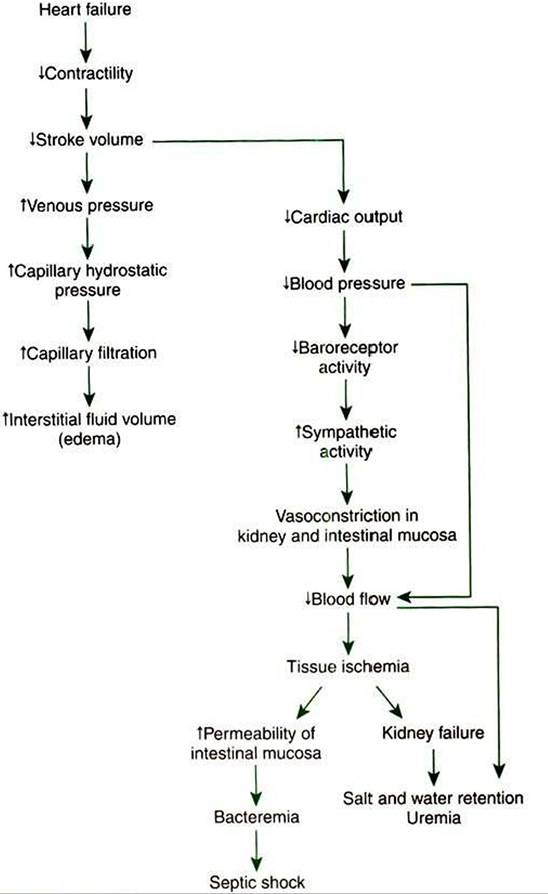
FIGURE 26-3 Heart failure leads to exercise intolerance. Additional, life-threatening complications secondary to heart failure are diagrammed here, including edema, salt and water retention, uremia, kidney failure, and septic shock. See text for details.
Whether the edema is in the lungs or in the systemic circulation, its degree is limited by the three safety factors previously discussed (see Figure 23-5). These safety factors would probably keep the edema of heart failure well controlled were it not for an additional factor that exaggerates the elevation of venous pressure in heart failure. As long as arterial pressure remains subnormal in a patient with heart failure, the baroreceptor reflex and some mechanisms involving the kidneys work to raise blood volume above normal. These volume-increasing mechanisms include increasing thirst (which raises fluid intake), increasing the release of antidiuretic hormone (ADH) from the pituitary (which decreases fluid loss in the urine), and activating the renin-angiotensin- aldosterone system (which decreases sodium loss in the urine). These effects of the baroreflex were mentioned briefly in Chapter 25, and the mechanisms involving the kidneys are described in more detail in Chapters 41 and 43.
The point for now is that the patient with severe heart failure experiences a substantial and persistent increase in blood volume. The excess blood accumulates particularly in the veins and capillaries upstream from the failing ventricle and often leads to an increase in capillary filtration that overwhelms the normal safety factors against edema. In fact, one of the main goals in the clinical treatment of heart failure is to counteract the buildup of excessive blood and interstitial fluid volume. Diuretic drugs are the main therapies used for this purpose (see Chapter 43).
Severe, persistent heart failure leads to several additional adverse effects. The baroreceptor reflex responds to an abnormally low arterial pressure in heart failure by initiating arteriolar vasoconstriction, primarily in the kidneys, splanchnic organs, and resting skeletal muscle (the “noncritical” organs). In severe failure the skin and mucous membranes are also vasocon- stricted. Vasoconstriction in these organs helps compensate for heart failure by permitting the available cardiac output to be routed to the “critical” organs (brain, heart, and working skeletal muscle). However, persistent vasoconstriction leads to the additional complications of uremia, kidney failure, and septic shock.
Vasoconstricted kidneys cannot form urine in a normal manner and therefore do not rid the body of the excess volume of blood and interstitial fluid that accumulates in heart failure. The compromised kidney function also allows nitrogenous and acidic waste products to accumulate in the body. The condition is called uremia, which literally means “urine in the blood.” To make matters worse, after a prolonged period of intense vasoconstriction, the kidney tissue becomes irreversibly damaged. At this stage, uremia, acidosis, and salt and water retention may persist even if clinical treatment is temporarily successful in returning cardiac output and blood pressure close to normal. In fact, renal failure often is the terminal event in chronic heart failure.
Intense and prolonged vasoconstriction in the splanchnic circulation can also have lethal consequences. The mucosa of the gastrointestinal tract is particularly susceptible to ischemic damage. Normally, the intestinal mucosa creates a barrier between the intestinal lumen and the bloodstream. Ischemic damage to the intestinal mucosa allows bacteria and bacterial toxins to pass into the bloodstream or the peritoneum. The resulting bacteremia or peritonitis can cause septic shock and death. The causes and consequences of renal and splanchnic ischemia are summarized in Figure 26-3 (bottom right).
Cardiac decompensation is an additional (and frequently terminal) complication secondary to heart failure. The basic concept of decompensation is that when heart failure reaches a certain degree of severity, the compensations by the body for heart failure end up making the heart failure worse. Vicious “decompensatory” cycles develop and can lead to death within a few hours unless there is vigorous medical intervention.
The specific mechanisms of the decompensatory cycles are very complex, but two examples illustrate the concept. As explained, in the case of left ventricular failure, the damming up of blood in the left atrium is compensatory because it increases left ventricular preload, which helps boost stroke volume back toward normal. However, the increased left ventricular preload leads to the secondary complication of pulmonary edema. If severe, pulmonary edema interferes with the oxygenation of blood. One tissue that depends critically on an adequate supply of oxygen is cardiac muscle; hypoxia depresses the contractility of cardiac muscle. Thus a vicious cycle can develop: severely depressed ventricular contractility → severe pulmonary edema -> inadequate oxygenation of blood → hypoxia of the left ventricular muscle, which further depresses ventricular contractility.
For a second example of a vicious decompensatory cycle, consider again the effects of the baroreflex on the kidneys.
Renal vasoconstriction is compensatory for heart failure in that it helps increase TPR, which helps raise arterial pressure back toward normal, which helps keep perfusion pressure high enough to deliver adequate blood flow to the critical organs. However, intense and prolonged renal vasoconstriction leads to the accumulation of acidic and nitrogenous waste products in the blood (uremia) and in various body tissues, including the heart. The accumulation of acidic and nitrogenous waste products in cardiac muscle tissue depresses cardiac contractility. Thus» another vicious cycle can develop: severe ventricular failure → intense and prolonged renal vasoconstriction → uremia → accumulation of metabolic waste products in cardiac muscle, which further depresses ventricular contractility.Other decompensatory cycles develop in cases of severe, prolonged heart failure, but these examples illustrate the basic concept and show why decompensation is such a serious development.
In summary, in addition to exercise intolerance, the lifethreatening complications secondary to heart failure include edema, salt and water retention, uremia, kidney failure, septic shock, and decompensation. Careful clinical diagnosis and prompt treatment of heart failure are imperative, even in cases in which compensatory mechanisms have maintained blood pressure near its normal level.
In evaluating the severity of heart failure and the extent of compensation, it is clinically useful to group the signs of heart failure into two categories. The first category is referred to as backward heart failure. The signs of backward heart failure include the changes in the circulation upstream from the failing ventricle: increased atrial pressure, increased venous pressure, excessive capillary filtration, edema, and the functional changes secondary to edema (e.g., respiratory failure). The category forward heart failure refers to the consequences of heart failure downstream from the failing ventricle: decreased cardiac output, decreased arterial blood pressure, and the consequences of excessive vasoconstriction in the systemic organs, especially the kidneys and intestines.
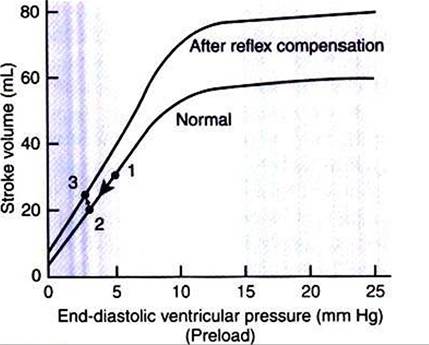
FIGURE 26-4 Direct effect of hemorrhage is to decrease ventricular preload, which decreases stroke volume (transition from point 1 to point 2). Stroke volume is restored toward normal by a reflex increase in sympathetic activity, which increases ventricular contractility above norma/(transition from point 2 to point 3).