Hemoglobin and Bicarbonate Are the Most Important Blood Buffers
Hemoglobin is an important blood buffer because it is plentiful and because the imidazole residues of globin histidine have a pKa close to the blood pH. In actuality, the pKa of hemoglobin changes with the degree of oxygenation.
Because deoxyhemoglobin has a pKa (7.93) closer to blood pH than does oxyhemoglobin (pKa = 6.68), deoxyhemoglobin provides more buffering capacity. When arterial blood enters the tissue capillaries, oxygen leaves hemoglobin, so the resulting deoxyhemoglobin is an excellent buffer for the H4 produced when CO2 is added to the blood.The other blood buffer with an optimal pKa is the HPO42- /H2PO4 system, with a pKa of 6.8 (see Figure 52-1). The normally low phosphate concentration in the blood makes this buffering system quantitatively unimportant; however, it is important in the renal tubules, where phosphate is concentrated. Plasma proteins also provide a small amount of blood buffering.
Although a pKa of 6.1 seems to make the HCO3TH2CO3 buffer unimportant for blood buffering, this is not so for two reasons. First, there is a large amount (24 mEq∕L) of HCO3" in the blood, making it readily available for buffering. Second, the kidneys can regulate the concentration of HCO3", and the lungs can regulate the concentration of H2CO3. Because the base and acid concentration can be regulated, the HCO3TH2CO3 system is said to be an open system.
Figure 52-2 shows the value of this open system in maintaining body pH. it should be noted that the concentration of H2CO3 ((H2CO3]) in solution is directly proportional to the carbon dioxide tension (Pco2); 1 molecule of H2CO3 is in equilibrium with 340 molecules of CO2.
Therefore, (H2CO3I is calculated as 0.03 ∙ Pco2. In Figure 52-2, A and B, top panels, 5 mmol of hydrochloric acid is added to plasma. Figure 52-2, A, shows what happens if the Pco2 and thus (H2CO3I is held constant. In such a closed system, the 5 mmol of HCl reacts with 5 mmol of HCO3" to form 5 mmol of H2CO3. As a consequence of this reaction, [HCO3"] decreases from 24 to 19 mmol∕L, (H2CO3) increases from 1.2 to 6.2 mmol∕L, and Pco2 increases from 40 to 206 mm Hg. Using the law of mass action, one can calculate that [H4] increases from 40 to 257 nEq∕I. or, stated in other terms, pH decreases from 7.4 to 6.5. If the system is open, however, as it is in the top panel of Figure 52-2, B, carbon dioxide evolves to the environment as fast as it is produced so that Pco2 and therefore [H2CO3] remain constant, then [H4] increases to only 50 nEq∕l. and the pH decreases only to 7.3. The lower panel in Figure 52-2, B, shows similar advantages to the open system when a strong base is added to the buffer system.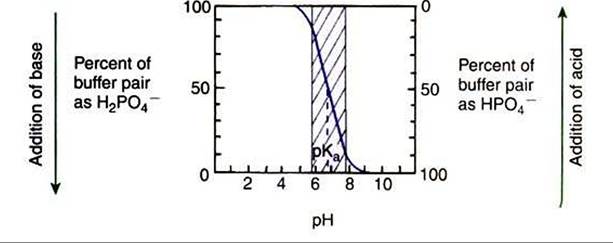
FIGURE 52-1 Titration curve for the phosphate buffer system. The pKit is 6.8. The shaded area represents the range of pH over which this buffer is effective.
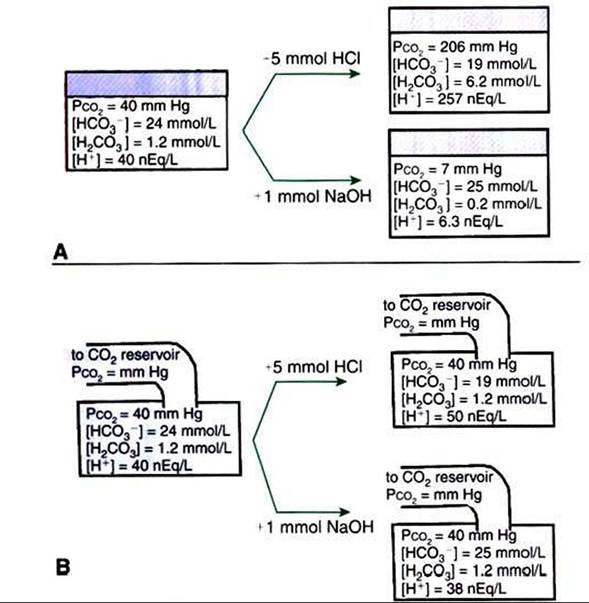
FIGURE 52-2 Buffer function of the carbonic acid-bicarbonate system under closed and open conditions. Ar Under closed conditions, the total quantity of the buffer (acid plus base components) remains constant. Br Under open conditions, the carbon dioxide tension (Pco2) of the system, and thus the concentration of carbonic acid (H2CO3), is maintained at a fixed level by continuous equilibration of the liquid phase with a gas reservoir of constant Pco2.The term [H2CO3] denotes the combined concentration of carbonic acid and dissolved carbon dioxide.
(FromMadias NE, Cohen JJ: Acid-base chemistry and buffering. In Cohen JJ, Kassirer JP, editors: Acid-base, Boston 1982, Little, Brown.)
Under most conditions» the body functions as an open system with regard to the HCO37H2CO3 system so that pH changes are minimized. When tissues are ischemic, however, they have no connection to the lungs, so CO2 cannot be eliminated. The ischemic tissue then functions as a closed system, and pH changes within the tissue can therefore be drastic.
The HCO3ZH2CO5 buffering system is of great value to clinicians because its components can be readily measured in the clinical laboratory and thereby used to diagnose acid-base disturbances. It is not necessary to measure the components of every buffering system to diagnose acid-base disturbances. If one system is known, changes in other systems can be predicted. It is standard to measure pH and Pco2 and to use the Henderson-Hasselbalch equation to derive [HCO5"). In actual practice, these calculations are now done for the clinician by computers in the blood gas machine.
For clinical use, the Henderson-Hasselbalch equation for the HCO37H2CO3 system is written as follows:
pH = pKa + log[HCO3 )/(0.03 ∙ Pco2j
Under normal conditions, the pH of arterial blood is 7.4, the concentration of HCOf is 24 mEq∕L, and the arterial carbon dioxide tension (Paco2) is equal to 40 mm Hg:

This equation demonstrates that a normal blood pH requires an [HCOf ]∕[0.03 ∙ Pco2] ratio of 20:1. An increase or decrease in this ratio increases or decreases pH, respectively.