Innervation and Vascularization
The most important nerves of the abdominal wall are the last thoracic (T13) and the first and second lumbar nerves, although the floor ventral to the costal arch is served by continuations of the caudal intercostal nerves.
A knowledge of the topography and distribution of the nerves to the flank is of practical importance in obtaining local anesthesia.The skin is divided into bands (dermatomes) that encircle the trunk, and each is the territory of a particular spinal nerve. The peritoneal regions supplied by spinal nerves correspond very closely to the dermatomes. The skin of the abdomen is supplied by branches from both dorsal and ventral primary rami, but the muscles and other deep structures are supplied by ventral rami alone (see Fig. 1.37). The dorsal rami (Fig. 1.37/4) of the thoracic and lumbar nerves supply the epaxial muscles and the strip of skin extending from the dorsal midline roughly to the level of the patella. Below this line the skin is supplied by two tiers of branches from the ventral rami (Fig. 1.37/5).
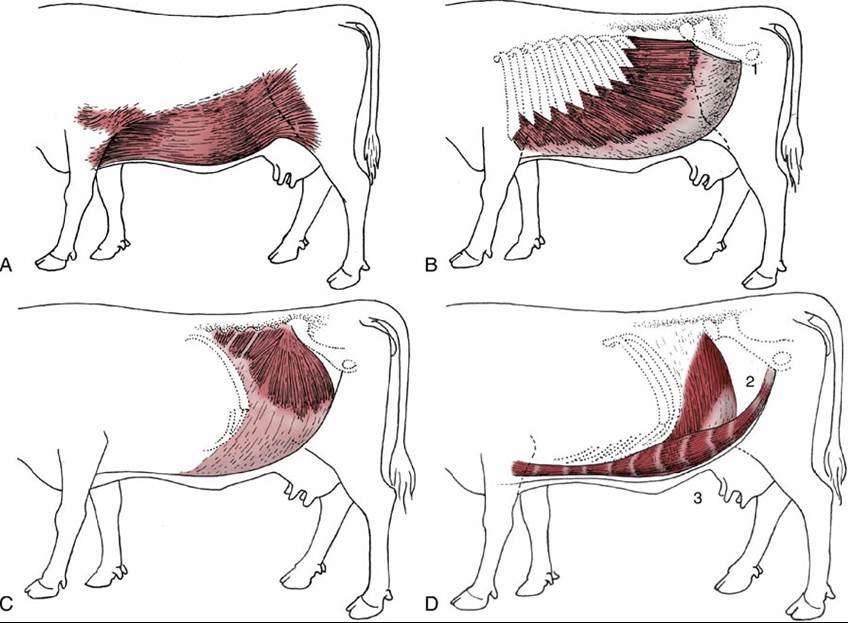
FIG. 28.1 Cutaneous trunci and abdominal muscles. (A) Cutaneous trunci, especially well developed ventrally. (B) External abdominal oblique with superficial inguinal ring (1) in its aponeurosis. (C) Internal abdominal oblique. (D) Transversus abdominis (2) and rectus abdominis (3). Note the reduction in the thickness of the wall along the caudal part of the rectus margin.
The ventral rami are much widened where they enter the flank between the internal oblique and transverse muscles. Each possesses a rather constant relationship to the skeleton that is a useful guide for blocking the nerves with anesthetics. These nerves run obliquely, deviating in an increasingly caudal direction (Fig. 28.2). The last thoracic ventral branch usually passes below the tip of the first lumbar transverse process, the first lumbar branch (iliohypogastric nerve) passes below the tip of the second, and the second lumbar branch (ilioinguinal nerve) passes below the tip of the fourth (Fig.
28.3). Most variations affect the last of these three nerves, which sometimes passes below the transverse process of the third lumbar vertebra.An exception to the general pattern of innervation of the abdominal wall is the nerve from the brachial plexus to the cutaneous muscle.
Incisions of the upper flank require blockage of both dorsal and ventral branches. Anesthesia is most conveniently obtained by paravertebral injection of the relevant nerves close to their foramina of emergence from the vertebral canal. Anesthesia of the lower flank and abdominal floor requires blockage of the ventral branches only, and these are most conveniently reached where they pass close to the tips of the lumbar transverse processes (paralumbar block). Variation in topography requires wider diffusion of the anesthetic agent for reliable effects. Lumbar epidural injection provides an alternative procedure. The specific innervation of the cutaneous muscle must be kept in mind regardless of the method chosen.
The abdominal wall receives blood vessels from several sources. The ventral part obtains its supply through the cranial and caudal epigastric arteries, which are branches of the internal thoracic and external pudendal arteries, respectively. The flanks are supplied from parietal branches of the aorta, of which the most important surgically is the deep circumflex iliac artery, which comes from the external iliac to pierce the flank a little cranial to the coxal tuber. The veins are initially satellite, but in the parous cow the arrangement is modified with the formation of the "milk" vein (p. 710).
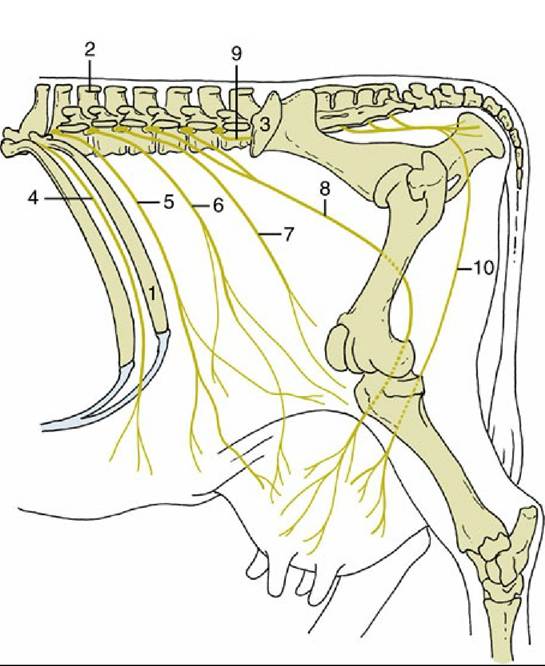
FIG. 28.2 Topography of the nerves to the flank and udder, simplified. The dorsal branches of the spinal nerves to the upper part of the flank are not shown. 1, Last rib; 2, spinous process of second lumbar (L2);
3, coxal tuber; 4, 12th thoracic (T12) (intercostal nerve [n.]); 5, T13 (costoabdominal n.); 6, L1 (iliohypogastric n.); 7, L2 (ilioinguinal n.); 8, L3 and L4 (genitofemoral n.); 9, L5 (nerve); 10, ventral perineal n.