Innervation, Vascularization, and Lymph Drainage of the Pelvic Walls
The branches of the lumbosacral plexus that traverse the pelvis are considered in detail on page 311, and only a few features are mentioned here. The obturator nerve follows the usual course over the medial aspect of the shaft of the ilium to reach the obturator foramen, and this exposes it to risk of injury in fractures of the bone or by compression during parturition (Fig.
22.4/15). The point of origin of the cranial gluteal, sciatic, and caudal gluteal nerves is exposed to similar risk where it lies against the ventral aspect of the sacrum, en route to the greater sciatic foramen (Fig. 22.4/13).The pudendal nerve (Fig. 22.4/12) arises from the middle sacral nerves (S[2]3-S4) and heads in the direction of the ischial tuber. The nerve first runs internal to the sacrosciatic ligament but later becomes embedded within its substance. As the nerve passes the lesser sciatic foramen, it exchanges fibers with the caudal cutaneous nerve of the thigh through the opening. With the main trunk continuing to the clitoris or the penis, the most important among its branches is the deep perineal nerve, which supplies the striated musculature of the perineum (Fig. 22.4/12'). The superficial branch is sensory to the anus, vulva, and perineal skin as far ventrally as the udder (or scrotum and prepuce).
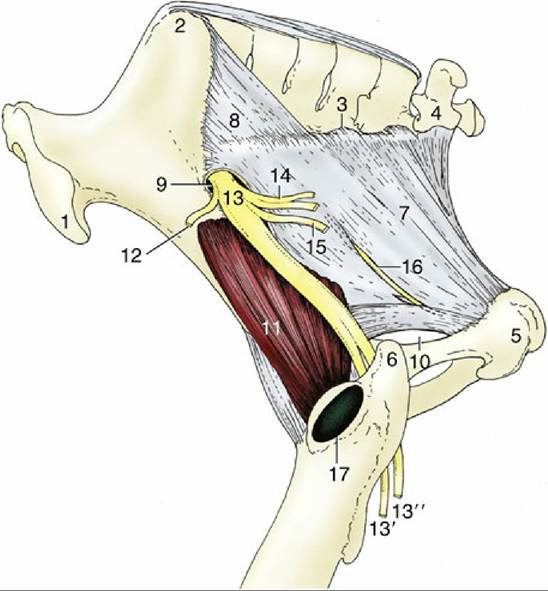
FIG. 22.1 Lateral view of the bony pelvis and sacrosciatic ligament. 1, Coxal tuber; 2, sacral tuber; 3, lateral border of sacrum; 4, caudal vertebra 1; 5, ischial tuber; 6, caudal part of greater trochanter; 7, sacrosciatic ligament; 8, dorsal sacroiliac ligament; 9, greater sciatic foramen; 10, lesser sciatic foramen; 11, gluteus profundus; 12, cranial gluteal nerve; 13, sciatic nerve; 13', common peroneal nerve; 13", tibial nerve; 14, caudal gluteal nerve; 15, caudal cutaneous femoral nerve; 16, pudendal nerve; 17, trochanteric bursa.
The caudal rectal nerve (Fig. 22.4/11), which arises from the same sacral nerves (S[2]3-S4), is motor to the striated muscles of the dorsal part of the perineum and sensory to the rectum, the wall of the anal canal, and adjacent skin.
The pelvic nerves (Fig. 22.4/14) are deployed in the usual fashion and are composed of parasympathetic fibers from the second, third, and fourth sacral nerves.
The blood supply to the pelvic contents and walls is attended to by the internal iliac arteries, terminal branches of the abdominal aorta (Fig. 22.4). The very short internal iliac artery passes below the wing of the ilium and soon divides into internal pudendal and caudal gluteal arteries. The internal pudendal artery has a mainly visceral distribution. It runs caudoventrally on the deep face of the sacrosciatic ligament, close to the pudendal nerve, before swinging medially to divide about the level of the ischial spine. Its branches include the umbilical artery, which conveys a little blood to the vertex of the bladder (and the adjacent part of the deferent duct in the male), and a much more important branch that supplies the bulk of the intrapelvic reproductive organs. This is known as the vaginal artery in the female, in which it supplies the greater part of the bladder, the urethra, the caudal part of the uterus, the vagina, and, by way of the middle rectal artery, a substantial part of the rectum. The homologous prostatic artery supplies the bladder, the urethra, the accessory genital glands, and the corresponding part of the rectum. End branches of the internal pudendal artery (Fig. 22.4/12') include the caudal rectal artery to the rectum and anus, a (ventral) perineal artery for the tissues between the anus and vulva, and branches to the vestibule and the vestibular bulb; the male counterpart of the last named is the artery of the penis, which anastomoses with divisions of the obturator.
The caudal gluteal artery passes caudally in the dorsolateral wall of the pelvis; it branches off the obturator and cranial gluteal arteries.
The trunk pierces the sacrosciatic ligament before supplying the hamstring muscles and the tail. The obturator artery leaves the pelvis through the obturator foramen, and the cranial gluteal artery exits through the greater sciatic foramen.The veins largely mirror the patterns of the arteries.
The lymph nodes associated with the pelvic walls display the usual species characteristics, comprising numerous, closely packed, and individually small nodes that aggregate to form sizable masses. The major groupings are related to the termination and parietal branches of the aorta. Sacral nodes lie between the divergent internal iliac arteries, medial iliac nodes lie at the origin (from the external iliac) of the deep circumflex iliac arteries, and lateral iliac nodes lie at the terminal division of the latter.
Other (anorectal) nodes lie over the caudal part of the rectum. In the horse the deep inguinal nodes (Fig. 22.4/4) lie outside the pelvic cavity, within the femoral triangle and at no great distance from the superficial inguinal nodes. The latter are interposed between the prepuce and scrotum (or udder) and the trunk. They drain lymph from the external reproductive organs (and udder) and from the skin and deeper structures over a considerable part of the ventral trunk. This lymph is then channeled to the deep inguinal nodes, which also receive most lymph from the hindlimb, of which a part has already been filtered through the nodes in the popliteal fossa. The outflow goes to the medial iliac nodes, which constitute the collecting center for lymph emanating from the caudal abdominal and pelvic walls and from the pelvic viscera. Much of this lymph has already passed through anorectal, sacral, or lateral iliac nodes. The outflow is either to the aortic lumbar nodes of the abdominal roof or directly to an erratically formed lumbar trunk.