» The Rectum and Anal Canal
The principal features of visceral topography and peritoneal disposition are shown in Figs. 22.5, 22.6, and 22.7.
The rectum continues the descending colon beyond the pelvic inlet.
Initially it resembles the colon in structure and in relationship to the peritoneum, but as it proceeds caudally the mesentery shortens and the peritoneal covering is gradually lost (commencing with the dorsal aspect); finally, the rectum is wholly retroperitoneal and embedded in a fat-rich connective tissue. The proportion of the rectum that is retroperitoneal appears to vary between individuals and is among to the perforations of the wall of the rectum that may occur during clinical procedures. The terminal part of the rectum loses the sacculated character and forms a wide flask-like expansion (ampulla) just before it joins the anal canal. The ampulla stores feces before evacuation. The regrouped dorsal and lateral longitudinal muscle bundles break free, pass above the anus, and anchor the rectum to the fourth or fifth caudal vertebra; these bundles constitute the smooth rectococcygeus (Fig. 22.4/9).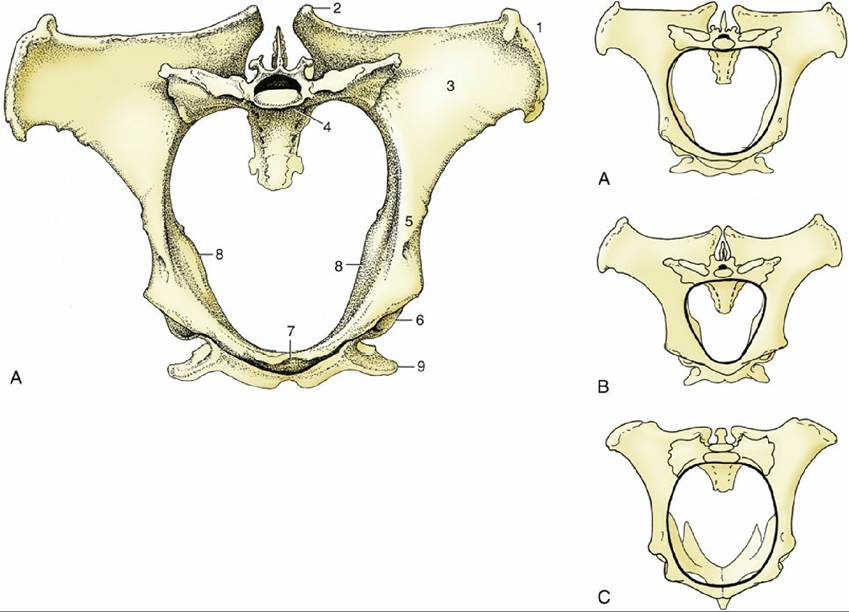
FIG. 22.2 Cranial view of the pelvis of the mare (A), stallion (B), and cow (C). The terminal line is emphasized in the smaller pictures; observe the differences in the shape of the pelvic inlet and position of the ischial spines. 1, Coxal tuber; 2, sacral tuber; 3, wing of ilium; 4, promontory; 5, shaft of ilium; 6, acetabulum; 7, brim of pubis; 8, ischial spines; 9, ischial tuber.
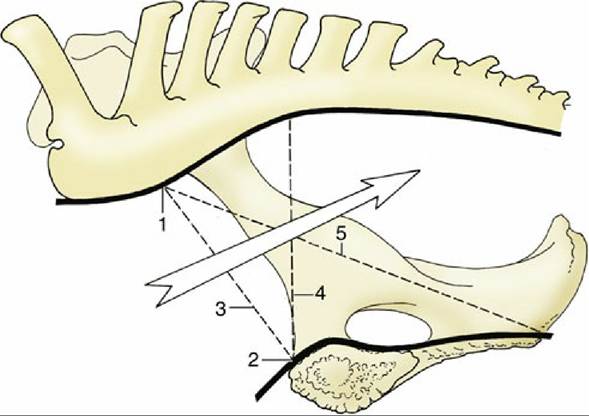
FIG. 22.3 Schematic median section of the mare's pelvis illustrating certain obstetric terms. 1, Promontory; 2, cranial end of the pelvic symphysis; 3, conjugata; 4, vertical diameter; 5, diagonal conjugata. The arrow indicates the axis of the pelvic canal.
The relations of the rectum depend on its fullness and on the sex. In the mare, the rectum lies on the uterus and vagina unless, as often happens, these are displaced to one side and the rectum is enabled to make contact with the bladder. In male animals the ventral surface lies on the bladder, the urethra, and the accessory reproductive glands; the extents of the individual contacts depend on the state of the bladder and the development of the glands, which are naturally smaller in the gelding.
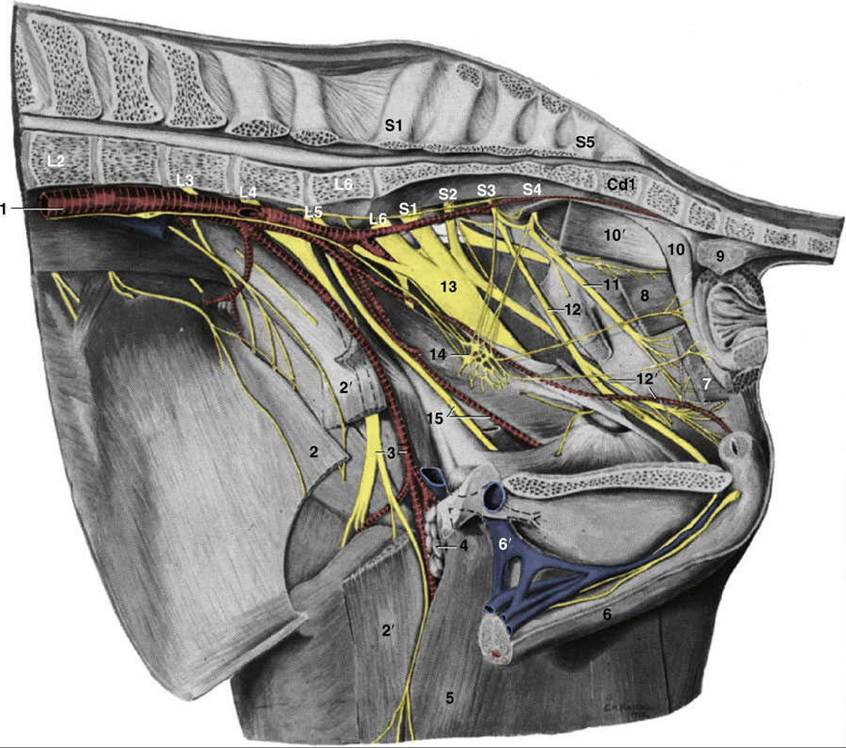
FIG. 22.4 Dissection of the pelvic wall, medial view. 1, Aorta; 2, internal abdominal oblique; 2', sartorius, resected; 3, femoral artery and nerve (n.); 4, deep inguinal lymph nodes; 5, gracilis; 6, penis; 6', (accessory) external pudendal vein; 7, levator ani, resected; 8, coccygeus; 9, rectococcygeus; 10, retractor penis; 10', ventral tail muscle; 11, caudal rectal n.; 12, pudendal n.; 12', deep perineal n. and internal pudendal artery; 13, sciatic n.; 14, pelvic plexus; 15, obturator n. and vessels. Cd1, caudal vertebra 1; L2-L6, second through sixth lumbar vertebrae; S1-S5, first through fifth sacral vertebrae.
The anal canal continues the rectum but, unlike this, is generally empty of feces. It is closed by the apposition and interdigitation of longitudinal mucosal folds and by the contraction of the internal and external anal sphincters. The extent of the canal is sharply defined by anorectal and anocutaneous lines marking the limits of epithelial specialization. The canal is embraced by the pelvic diaphragm (Fig. 22.4/7 and 8); the part caudal to the pelvic diaphragm projects as a cylindrical eminence within the perineal region.