Murmurs Are AbnormaI Heart Sounds Caused by Turbulent FIowThrough Cardiac Defects
Cardiac murmurs are abnormal heart sounds, and they often indicate the presence of cardiac abnormalities. Some murmurs are abnormalities in the first or second heart sound; others are additional (“extra”) heart sounds.
Murmurs are caused by turbulent flow through cardiac defects. The underlying physical principle is that laminar or smooth flow of blood through the heart or blood vessels is quiet, whereas turbulent flow is noisy. An analogy is that a river does not make any sound as it flows smoothly through a broad, relatively flat channel. If the same river enters a channel that is restricted or drops steeply, a rapid or cataract forms. The flow becomes turbulent, and the turbulent flow makes noise.The flow of blood through the heart and blood vessels is normally smooth, and therefore quiet, during all parts of the cardiac cycle, except two. The first moment of turbulent flow occurs at the beginning of ventricular contraction, on closure of the AV valves. The second moment of turbulent flow normally occurs at the end of ventricular systole, when the aortic and pulmonic valves close. The momentary turbulence and vibration associated with valve closure create the first and second heart sounds. Figure 21-1 indicates that the first heart sound is associated with the closure of the AV valves at the beginning of ventricular systole. The second heart sound is associated with the closure of the aortic and pulmonic valves at the end of ventricular systole. On occasion, normal third and fourth heart sounds are faintly audible with the stethoscope. In comparison, clinically important murmurs are louder. Sometimes, murmurs are even louder than the normal first and second heart sounds.
Table 21-2 lists cardiac valve defects that cause additional instances of turbulent flow and therefore murmurs. The table also indicates the timing of the murmurs in relation to the cardiac cycle.
Systolic murmurs occur during ventricular systole; diastolic murmurs occur during ventricular diastole. Continuous murmurs occur during both systole and diastole. The timing of each murmur is easy to remember if two basic principles are kept in mind: murmurs are caused by turbulent blood flow, and blood flows in response to pressure differences. In other words, turbulent (noisy) flow through a cardiac defect occurs only if there is a substantial pressure difference from one side of the defect to the other.Figure 21-8 indicates how these principles can be used to account for systolic murmurs. The numbers in the figure indicate the maximal pressures that normally exist in each cardiac chamber during ventricular systole. Note, for example, that the pressure in the left ventricle is normally much higher than the pressure in the left atrium during ventricular systole. The mitral valve is normally closed during ventricular systole, so no blood flows backward from the ventricle to the left atrium. If the mitral valve fails to close completely during ventricular systole, however, the large pressure difference between the left ventricle and the left atrium causes a rapid, backward flow of
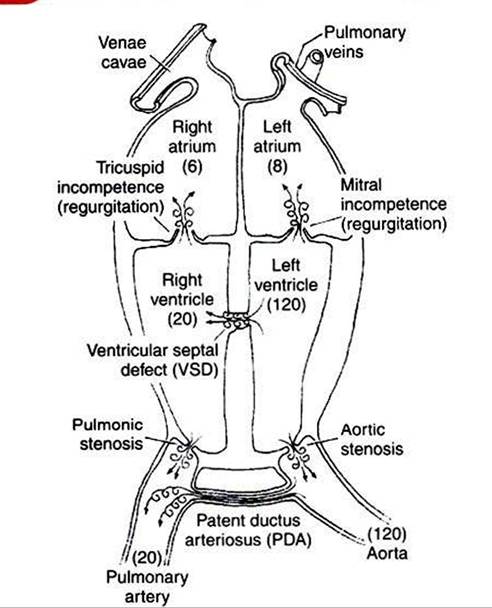
HGUKt 21-8 Schematic view of the heart showing cardiac defects that cause systolic murmurs.The numbers in parentheses indicate normal maximal pressures (mm Hg) during ventricular systole.The swirled arrows indicate the sites of turbulent (noisy) flow.
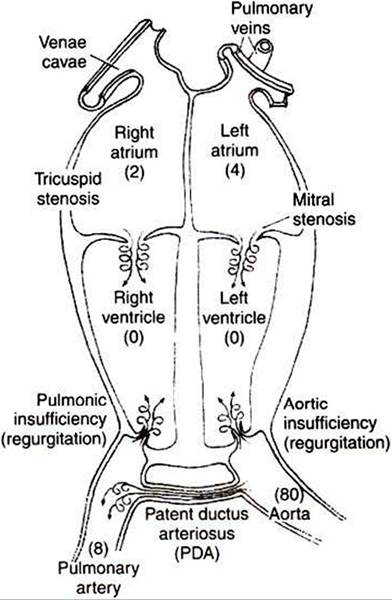
FIGURE 21-9 Cardiac defects that cause diastolic murmurs.The numbers in parentheses indicate normal minimal pressures (mm Hg) during ventricular diastole.The swirled arrows indicate the sites of turbulent (noisy) flow.
blood through the partially closed valve. This turbulent back- flow creates a systolic murmur. A mitral valve that fails to close completely is said to be insufficient or incompetent.
The back- flow across the valve is called regurgitation. Mitral regurgitation is present in about 8% of dogs over 5 years of age.A ventricular septal defect (VSD) is a hole or cleft in the interventricular septum. Blood flows through a VSD from the left ventricle to the right ventricle during ventricular systole because systolic pressure is much higher in the left ventricle than in the right ventricle. Typically, the flow of blood through a VSD is turbulent, and a systolic murmur is created.
Systolic turbulence is also created if the aortic valve does not open widely enough. Blood ejected from the ventricle accelerates to a high velocity as it squeezes through the restricted aortic opening, and turbulence occurs. A valve that fails to open widely enough is called stenotic; the defect of aortic stenosis produces a systolic murmur. Likewise, pulmonic stenosis causes a systolic murmur. Aortic and pulmonic stenosis are common congenital defects in dogs.
A patent ductus arteriosus (PDA) is persistence after birth of the opening between the aorta and the pulmonary artery (see Chapter 51). A PDA produces a murmur during systole because the pressure in the aorta is much higher than the pressure in the pulmonary artery. Blood flows from the aorta into the pulmonary artery, and turbulence occurs. The murmur of a PDA is not restricted to systole, however, because the aortic pressure remains higher than the pulmonary artery pressure throughout diastole. Therefore the murmur of PDA is heard in both systole and diastole and is thus a continuous murmur. It is also called a machinery murmur because it characteristically sounds like the rumble of machinery. PDA is common in dogs, especially females.
The site on the thorax from which a particular murmur can be heard (auscultated) best is often indicative of the particular location and type of defect that causes the murmur. For example, the murmur of PDA is characteristically heard best over the left heart base.
Occasionallv, the turbulence caused by a cardiac defect will be so extreme as to cause a palpable thoracic vibration (thrill).Animals sometimes have open pathways for blood flow between peripheral arteries and peripheral veins. These openings are called arteriovenous fistulae. Arteriovenous fistulae carry flow (and create turbulence) during both systole and diastole and therefore create continuous murmurs. The murmur of an arteriovenous fistula is most audible at the body surface close to the point of the fistula.
The numerical values in Figure 21-9 correspond to the minimal pressures that normally exist in the various cardiac chambers during ventricular diastole. These pressures form the basis for understanding why certain cardiac defects typically produce diastolic murmurs. For example, a normal mitral valve opens widely during ventricular diastole, which creates a low-resistance pathway for blood to flow from the left atrium into the left ventricle. However, if the mitral valve fails to open widely (mitral stenosis), ventricular filling must occur through a stenotic (narrow) valve. This creates turbulent flow and a diastolic murmur. Mitral stenosis is a common murmur among humans who have developed calcification of the mitral valve as a result of rheumatic heart disease.
During diastole the normal aortic valve is closed» and no blood flows backward from the aorta into the left ventricle. If the aortic valve does not close tightly, blood flows backward (regurgitates) from the aorta to the left ventricle during diastole. Therefore, aortic regurgitation produces a diastolic murmur. The defect is called aortic incompetence or aortic insufficiency. Aortic regurgitation is common in horses but not in dogs.
Diastolic murmurs can also be produced by defects on the right side of the heart. Pulmonic regurgitation produces a diastolic murmur, but it is relatively rare. Tricuspid stenosis is uncommon, at least as a congenital defect. However, a heavy infestation of heartworms in the right side of the heart can create a stenosis at the tricuspid valve and a diastolic murmur.
Cardiac murmurs themselves are not harmful. They are clinically important, however, because the defects that cause the murmurs also cause pathological changes. Cardiac defects typically lead to one or more of these pathological consequences: (1) abnormally high or low blood flow to a region of the body, (2) abnormally high or low blood pressure in a region of the body, and (3) cardiac hypertrophy (enlargement of cardiac muscle).
It is not difficult to understand why cardiac defects lead to abnormal blood flows or abnormal blood pressures. For example, in the presence of a ventricular septal defect, the right ventricle receives blood from both the right atrium and the left ventricle, which leads to an abnormally high blood flow through the pulmonary circulation. In the presence of aortic stenosis, the left ventricle must generate an abnormally high systolic pressure to eject blood through the narrow valve opening. In the presence of mitral stenosis, blood dams up (and excessive pressure builds up) in the left atrium and pulmonary veins. It is more difficult to understand why some cardiac defects lead to cardiac hypertrophy. The underlying principle is that some cardiac defects increase the workload of one or both ventricles, and an increase in the workload of cardiac muscle leads to hypertrophy. Developing this concept more fully requires an understanding of cardiac energetics, as described next.