Increasing the Heart Rate Does Not Increase Cardiac Output Substantially Unless StrokeVoIume Is Maintained
Because cardiac output is equal to stroke volume multiplied by heart rate, cardiac output might be expected to be proportional to heart rate; that is, doubling the heart rate would be expected to double cardiac output (Figure 21-6, dashed line).
However, if the heart rate is experimentally increased above its normal level with an electrical pacemaker, cardiac output increases somewhat, but not in proportion to the increase in heart rate. The reason, as mentioned earlier, is that diastolic filling time is reduced at high heart rates. The resulting reduction in end-diastolic volume reduces stroke volume, so cardiac output does not increase in proportion to heart rate (Figure 21-6, lower solid line). In fact, at heart rates greater than about 160 beats/min, stroke volume decreases so much that cardiac output actually declines with further increases in heart rate. This problem was encountered when early versions of artificial cardiac pacemakers malfunctioned in ways that caused high ventricular rates. Decreases in stroke volume at high heart rates are also encountered in certain cardiac arrhythmias. In paroxysmal atrial tachycardia, for example, a rapid heart rate is originated by an ectopic atrial pacemaker. The tachycardia occurs typically in bursts or paroxysms. The high heart rate limits diastolic filling so much that cardiac output falls below normal. This causes the blood pressure to fall so low that the patient becomes lethargic and may even faint.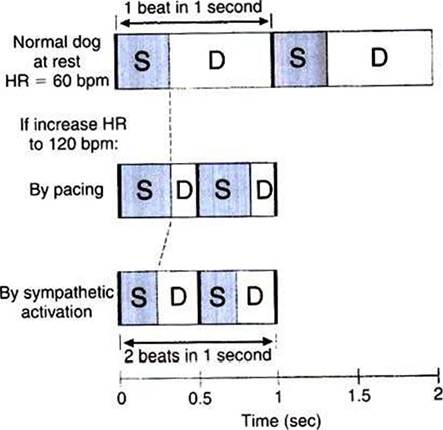
FIGURE 21-7 How shortening of systole (by sympathetic activation) helps to preserve diastolic filling time. Top, In a resting dog with a heart rate (HR) of 60 beats per minute (bpm), systole (S) takes about one-third second, leaving two thirds of each beat for diastole (D) and filling. Middle, If HR is increased to 120 bpm by an artificial pacemaker, the duration of systole is unchanged, so diastolic duration (filling time) is greatly reduced.
Bottom, If the same increase in heart rate is brought about by sympathetic activation, systole becomes shorter, which restores part of the lost diastolic filling time.Although cardiac pacing does not cause a large increase in cardiac output, increases in heart rate in the course of normal daily activities are accompanied by substantial increases in cardiac output. An example is the increase in cardiac output that normally accompanies exercise. As shown in Figure 21-6 (upper solid line), the actual increase in cardiac output during progressively more intense exercise is even greater than would be expected on the basis of the associated increase in heart rate. The reason that cardiac output increases so much during exercise is that stroke volume also increases. During exercise, increases in heart rate are brought about by increases in sympathetic activity. This sympathetic activation also increases cardiac contractility, so the ventricles empty more completely with each beat. In addition, sympathetic activation shortens the duration of systole, which helps to preserve diastolic filling time. In summary, under sympathetic action, the heart not only contracts more frequently (increased rate) and more forcefully (increased contractility), but also contracts and relaxes more quickly.
Figure 21-7 illustrates how the shortening of systole helps to preserve diastolic filling time. When heart rate is 60 beats/min, each beat takes 1 second. This 1 second must include one systole and one diastole. Typically, systole lasts about ⅛ second, which leaves 2A second (plenty of time) for diastolic filling. It heart rate is increased to 120 beats/min, each beat lasts only 1A second. Ifsystole remains at 1A second, there is only 1∕6 second left for diastolic filling (not enough time). However, if the increase in heart rate occurs because of an increase in sym-
Table 21-1
Typical Cardiac Changes During Vigorous Exercise in a Large Dog
| Measurement | Rest | Exercise |
| Ventricular end-diastolic volume ImL) | 60 | 55 |
| Ventricular end-systolic volume (mL) | 30 | 15 |
| Stroke volume (mL) | 30 | 40 |
| Ejection fraction (%) | 50 | 73 |
| Heart rate (beats/min) | 80 | 240 |
| Cardiac output (L√min) | 2.4 | 9.6 |
Table 21-2
CardiacVaIve Defects and Resulting Murmurs
| Site of defect | Nature of defect | |
| Incompetence or insufficiency (allows regurgitation) | Stenosis (narrow valve opening, creates restriction) | |
| Atrioventricular valves | Systolic murmur | Diastolic murmur |
| Aortic or pulmonic valves | Diastolic murmur | Systolic murmur |
pathetic activity» systole becomes shorter, which restores part of the lost diastolic filling time.
Diastole is shorter under these conditions than at rest, but it is longer than it would have been if systole were not shortened. Thus, sympathetic activation is said to help preserve the diastolic filling time. Overall, sympathetic activation (especially when coupled with a decrease in parasympathetic activity) can dramatically increase cardiac output (Table 21-1).It is useful at this point to review the control of cardiac output, as summarized in Figure 21-2. Cardiac output is determined by stroke volume and heart rate. Stroke volume is determined by end-diastolic volume and end-systolic volume. End-diastolic volume depends on preload, ventricular compliance, and diastolic filling time. End-systolic volume depends on contractility and, to a lesser extent, on arterial pressure or afterload (not shown in Figure 21 -2). Sympathetic activation increases contractility. Heart failure decreases contractility, as do several drugs often used in veterinary practice. Increased heart rate acts directly to increase cardiac output, but it also decreases diastolic filling time, which compromises the increased cardiac output. Heart rate is increased by sympathetic activation and parasympathetic withdrawal. Sympathetic activation also shortens systolic duration, which helps to preserve diastolic filling time.