Parasympathetic system
Key points
■ Presynaptic parasympathetic LMNs originate in the craniosacral CNS, such as from brainstem nuclei and the sacral spinal cord.
■ Postsynaptic nerves originate in ganglia that are situated close to/within the organ they are innervating.
■ Parasympathetic nuclei III, VII, IX and X innervate the head. Additionally the vagus nerve (CN X) also innervates the viscera of the thorax and abdomen. Sacral parasympathetic nerves innervate pelvic viscera.
The parasympathetic or craniosacral system originates from the cranial end of the CNS (brainstem) in the parasympathetic nuclei of III, VII, IX, X and the intermediate horn of the sacral (S1-S3) spinal cord.
Supply to the head
Cranial nerves III, VII, IX and X supply the head as noted in Table 12.2 and Chapter 10. The vagus nerve, CN X is named for its long, wandering course (vagus - L = wandering). The vagus nerve contains a high proportion of visceral afferent fibres as well as visceral efferent fibres. For example, the cervical portion of the vagus nerve is estimated to be 80% visceral afferent (C type) fibres. Afferent fibres from the head and body have their unipolar sensory nerve cell bodies located in the proximal and distal vagal ganglia, respectively. The ganglia are sited in the jugular foramen (caudoventral inside the neurocranium) and near the tympano- occipital fissure; this fissure is located just caudal to the tympanic bulla on the caudolateral aspect of the base of the skull. Efferent fibres originate from the parasympathetic nucleus of X in the medulla oblongata. The efferent fibres leave the medulla oblongata bilaterally as rootlets in conjunction with somatic fibres of CN IX and CN XI. The caudally directed vagus nerve joins the cranially directed sympathetic trunk, to form the vagosympathetic trunk. The cranial laryngeal nerve exits the vagus at the base of the skull while the recurrent laryngeal nerve exits it in the cranial thorax; they innervate the larynx and oesophagus (see Fig.
10.19).Table 12.2 Parasympathetic (PS) innervation of the head
| Target organ and function | Origin | Ganglion and location | Pathway |
| Irts and lens of eye Pupilary l>ghτ reflex and accommodation | PS nucleus of CN III in midbrain | Oltary ganglion Just caudal to the eye | With somatic motor fibres of the oculomotor nerve |
| Lacrimal gland Smooth muscle of the nasal and oral cavities Tear and mucous membrane secretion | PS nucleus of CN Ml in rostral medula oblongata | Pterygopalatine gangion located on the pterygoid muscles | With SbresofCNVandCNVII |
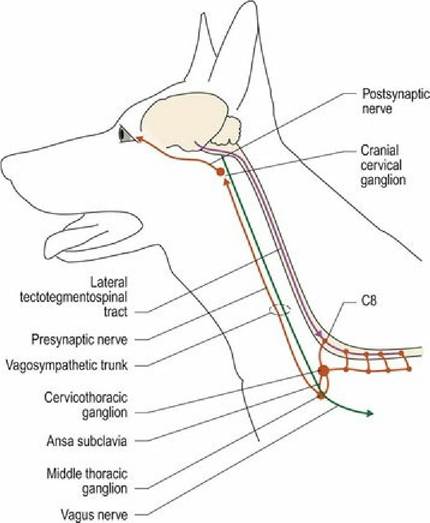
| Subllngual and mandibular salivary glands, glands cf of the rectum. These fibres then expand to form the pelvic plexus, which also receives sympathetic fibres via the hypogastric nerve. Both types of autonomic fibres are distributed to the pelvic viscera and reproductive organs. Fibres from the sacral parasympathetic supply have been traced through the length of the large intestine. Autonomic innervation of the eye Key points ■ Parasympathetic LMN innervation to the constrictor muscles of the iris originates in the midbrain, travels with the oculomotor nerve and has its postsynaptic neuron in the ciliary ganglion. It forms the efferent part of the pupillary light reflex. ■ Sympathetic LMN innervation of the dilator muscles of the iris originates in cranial thoracic cord. Presynaptic axons travel cranially in the vagosympathetic trunk, synapse in the cranial cervical ganglion and are distributed to the eye. ■ Loss of sympathetic input to the eye results in ‘Horner’s syndrome’ (ptosis, miosis, enophthalmos and protrusion of the third eyelid). It can also affect blood flow and glandular secretion in the head.■ Lesions of the midbrain can cause ‘fixed, dilated pupils’ due to damage to the parasympathetic nucleus of III. ■ Denervated smooth muscle is hypersensitive and responds to low concentrations of neurotransmitter. Consequently, dilute concentration of drugs that mimic ANS neurotransmitters, can be used to determine the site of an autonomic lesion. Parasympathetic innervation of the eye Bilaterally, the presynaptic neuron originates in the parasympathetic nucleus of III in the midbrain. These parasympathetic fibres mingle with the oculomotor nerve fibres arising from the oculomotor nucleus of the midbrain. The combined fibres emerge from the ventral aspect of the midbrain as CN III, the oculomotor nerve (Fig. A3). The parasympathetic fibres are located superficially on the medial side of the nerve where they are particularly susceptible to compression from any swelling or distortion of the midbrain. The nerve passes through the orbital fissure, into the periorbita and the parasympathetic fibres synapse in the ciliary ganglion close to the eyeball, just ventral to the optic nerve. The short, postsynaptic ciliary nerves travel to the eyeball and primarily innervate the smooth muscle constrictor of the pupil. The parasympathetic fibres of CN III form the efferent component of the pupillary light reflex (see Chapter 10). DysfUnction of the pupillary light reflex The clinical signs depend upon where the lesion is located and whether it is in the afferent portion of the reflex arc or the efferent portion. Determining the location is done by applying the primary concept of lesion localisation (see Fig. 13.1) that is by identifying whether other nearby neural pathways are functioning normally or are dysfunctional. Thus, if the lesion is located in the afferent portion of the reflex, then vision may be compromised (uni- or bilaterally). If the lesion is specifically located in the efferent portion of the reflex, then vision may be normal while the oculomotor function may also be compromised, resulting in strabismus. Sympathetic innervation of the eye Upper motor neurons travel caudally from the midbrain as the tectotegmentospinal tract to synapse on presynaptic LMNs in the cranial thoracic cord (C8-T5/7). The LMN axons pass through the cervicothoracic and middle cervical ganglia, cranially along the vagosympathetic trunk to synapse in the cranial cervical ganglion near the tympanic bulla. From there they travel with the internal carotid artery and then the ophthalmic branch of the trigeminal nerve to the eye (Fig. 12.5). Sympathetic innervation supplies the smooth muscle of the orbit, the upper eyelid and the iridal dilator muscles. Sympathetically induced, smooth muscle tone keeps the eyeball protruded, the palpebral fissure widened, the third eyelid retracted and pupils dilated. In stressful situations in which the sympathetic nervous system activity is increased, pupillary dilation is stimulated both by the sympathetic innervation and circulating adrenaline; the latter accounts for sustained effects of sympathetic stimulation on the eyes, blood vessels and viscera. Sympathetic stimulation causes increased visual acuity, increased blood flow to postural and locomotory muscles and increased heart and respiratory function.
Fig. 12.5 Sympathetic innervation of the eye.
More on the topic Parasympathetic system:
-
Veterinarian -
|