Regardless of the Status of Arterioles, Mechanical Compression Can Reduce Blood Flow to a Tissue
Mechanical compression can reduce blood flow in a tissue by literally squeezing down on all its blood vessels. The example of brief mechanical compression of the epithelial blood vessels has been mentioned as a way to trigger a readily visible reactive hyperemia.
Long-term mechanical pressure on the skin must be avoided, however, because a prolonged period of subnormal blood flow (ischemia) leads to irreversible tissue damage and cell death (infarction). Pressure sores are an unfortunate and common example. Three other specific instances of mechanical compression are also described because of their clinical importance.Figure 24-5 illustrates the effect of mechanical compression on coronary blood flow. The top tracing shows the changes in arterial (aortic) blood pressure during one complete cardiac cycle and the beginning of a second one. The periods of ventricular systole and ventricular diastole are labeled at the bottom of the figure. One would expect that left coronary blood flow would be highest during ventricular systole (when the aortic pressure is highest) and lowest during diastole (when the aortic pressure is lowest). However, the tracings of left coronary blood flow indicate that blood flow is actually depressed during systole and much higher during diastole. Flow even reverses (blood flows backward, toward the aorta) momentarily near the beginning of systole. The fact that coronary blood flow is much lower during systole, even though the perfusion pressure is higher, implies that coronary resistance must be substantially higher during systole than during diastole.
Coronary resistance is high during systole because the contracting ventricular muscle squeezes down on the coronary blood vessels, which increases their resistance to blood flow. The coronary vessels are not constricted in this way during diastole because the ventricular muscle is relaxed.
'Fherefore, coronary vascular resistance decreases dramatically (and blood flow increases) during diastole. The bottom tracing in Figure 24-5 indicates that mechanical compression has relatively little influence on right coronary blood flow. That is, the magnitude of right coronary blood flow closely follows the changes in arterial pressure (being highest during systole and lowest during diastole). The right ventricle contracts with much less force than the left ventricle, which explains why right coronary flow is not restricted by mechanical compression during systole. The right ventricle simply does not develop sufficient compressive force to constrict its own blood vessels.Most of the blood that is needed to support left ventricular metabolism must be delivered during ventricular diastole, when the vessels are not compressed. This fact has great clinical significance. In a resting animal with a low heart rate, there is adequate time during diastole for the coronary vessels to supply the amount of blood needed by the ventricular tissue. During exercise, heart rate and cardiac contractility both increase, which greatly increases the metabolic rate of the ventricular muscle cells. To support the increased metabolic rate, the ventricular tissue needs much more blood flow than at rest. However, the duration of diastole is reduced during exercise, so there is less time available for delivery of this increased flow. Nevertheless, normal, healthy coronary vessels have a sufficiently low resistance during diastole to supply the needed blood flow, even during maximal exercise. The situation is different, however, in animals with coronary artery disease. In animals whose coronary vessels are narrowed because Ofatherosclerosis, blood flow cannot increase enough to supply the needs of the vigorously working ventricular muscles. This is why ventricular ischemia develops during exercise in patients with coronary artery disease. Ischemic areas of the ventricle fail to contract normally.
Ischemia can also cause arrhythmias or even ventricular fibrillation (sudden death). Coronary artery disease is more common in humans than in veterinary species, so this scenario is more likely to occur in the veterinarian than in the veterinarian’s patients.Mechanical compression caused by muscle contraction can also restrict blood flow through skeletal muscles. The blood vessels within skeletal muscles become compressed during strenuous, sustained contractions of the muscle. The compression reduces blood flow and can create ischemia. Ischemic muscles cannot contract with normal vigor. Ischemia also activates sensory nerve endings in the muscle, which causes pain. Activation of these muscle ischemia receptors also triggers a reflex increase in arterial pressure. The high arterial pressure is advantageous because it partially overcomes the effects of mechanical compression on blood flow. In other words, a high arterial pressure helps to force blood flow through the skeletal muscle blood vessels, despite the compressive effects of the muscle contraction. The high arterial pressure of ischemic exercise is risky for patients with coronary artery disease, however, because high arterial pressure causes a tremendous increase in the cardiac workload. This is why patients with coronary artery disease are cautioned against types of exercise that involve strenuous, sustained muscle contractions, such as weightlifting.
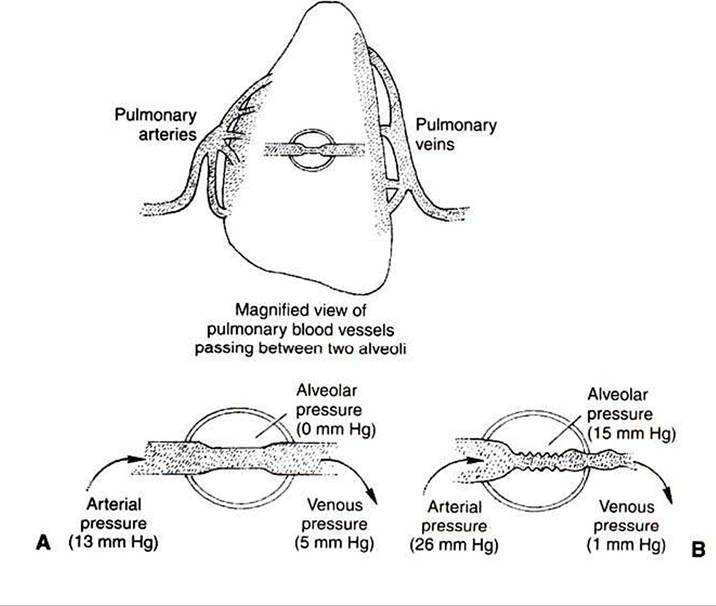
FIGURE 24-6 Pulmonary vessels are susceptible to mechanical compression.
A, Normally, pulmonary arterial and venous pressures are both higher than alveolar pressure, so pulmonary vessels stay open.
B, If alveolar pressure increases to 15 mm Hg or higher, however, the pulmonary blood vessels are compressed. The resulting increase in pulmonary vascular resistance causes pulmonary blood flow to decrease, pulmonary arterial pressure to increase, and pulmonary venous pressure to decrease.
Mechanical compression has important effects on the pulmonary circulation. Pulmonary arterial pressure is much lower than systemic arterial pressure, so mechanical compression can easily reduce pulmonary blood flow, as illustrated in Figure 24-6. This diagram shows a pulmonary blood vessel passing between two alveoli. Under normal conditions the arterial pressure is 13 mm Hg and the venous pressure 5 mm Hg (Figure 24-6, A). The pressure just outside the vessels (i.e., in the alveolar air spaces) is even lower; alveolar pressures typically vary between -1 mm Hg (during inspiration) and +1 mm Hg (during expiration). Because the pressure inside pulmonary vessels is greater than the pressure outside, the vessels are not compressed.
Figure 24-6, B, depicts a compression of pulmonary blood vessels resulting from an abnormally high alveolar pressure. This could happen during surgery if a patient has a tracheal tube inserted into the airway and the tracheal tube is attached to a source of elevated pressure. The elevated pressure could be generated by a mechanical respirator that is not adjusted properly or by an anesthetist when he or she squeezes the bag that is attached to the tracheal tube. In either case, the pressures generated in the tracheal tube are transmitted to the alveoli. An increase in alveolar pressure increases the external compressing pressures applied around the pulmonary blood vessels.
Alveolar pressures exceeding 10 to 15 mm Hg compress pulmonary blood vessels sufficiently to raise the resistance to blood flow through the lungs. Pulmonary blood flow decreases. Two events occur as a result. First, less blood reaches the left atrium and left ventricle, which causes left ventricular stroke volume and aortic blood pressure to decrease. Second, blood ejected by the right ventricle dams up in the pulmonary arteries. This causes pulmonary arterial pressure to increase. An elevated pulmonary arterial pressure helps force blood through the compressed vessels. However, the increased pulmonary artery pressure also places an increased workload on the right ventricle. If the alveolar pressure is not excessively high, the right ventricle generates sufficient pulmonary arterial pressure to restore pulmonary blood flow almost to normal. However, with extremely high alveolar pressures, the right ventricle is unable to raise pulmonary arterial pressure high enough to sustain flow. Under these conditions, pulmonary blood flow and thus systemic blood flow fall substantially below normal, and systemic hypotension and ischemia develop in the patient. The consequences can be fatal. The veterinary clinician must be mindful of the risks of high airway pressures whenever a patient is intubated and attached to a mechanical respiratory device.