Respiratory Acidosis Is Caused by the Accumulation of Carbon DioxiderWhich Decreases Blood pH
Respiratory acidosis is caused by alveolar hypoventilation, which can result from damage to or depression of the respiratory control centers, injury to the respiratory pump (e.g., fractured ribs, bloated abdomen), or severe respiratory disease that either obstructs the airways or excessively stiffens the lungs.
When alveolar hypoventilation occurs, Pco2 increases because carbon dioxide is incompletely eliminated by the lungs. The reaction:
is driven to the right by the accumulating CO2; H accumulates, and pH decreases. Bicarbonate accumulates simultaneously, but the amount is too small to keep the [HC0370.03 ∙ PCO2J ratio at a normal value of 20:1.
In the blood, other nonbicarbonate buffers not only take up H+ produced by the accumulation of CO2 but also assist in the accumulation of HCOt, as follows:
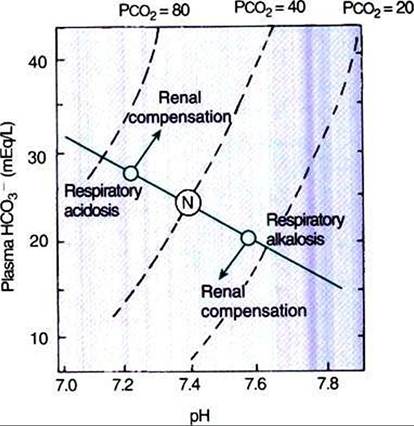
FIGURE 52-4 A pH-bicarbonate diagram showing the effects of respiratory acidosis and alkalosis on pH, bicarbonate (HCO3 ) concentration, and carbon dioxide tension (Pco2) of arterial blood. In acute respiratory acidosis, as Pco2 increases, the changes in pH and bicarbonate concentration are predicted by the normal buffer line. Renal compensation leads to an accumulation of HCO3', which increases the pH, whereas Pco2 remains constant. In respiratory alkalosis, Paco2 and HCO3 decrease and pH increases. The kidneys compensate by increasing HCO3 resorption, which decreases pH. Λ∕z Normal arterial blood composition.

By buffering H+, hemoglobin (Hb-) pulls the first reaction to the right and produces HCO3-.
This accumulation of bicarbonate, shown on the normal buffer line in the pH-HC03- diagram (see Figure 52-3), is still insufficient to maintain a normal (HC0370.03 ∙ Pco2] ratio, and therefore the pH decreases. As a result of these various reactions, the characteristic findings in acute respiratory acidosis are an elevated Paco2, a decreased pH, and a minor increase in [HCO3-].To facilitate the clinical interpretation of acid-base status, clinicians use the terms total buffer base, base excess, and base deficit. Total buffer base is the sum of the concentrations of available blood buffers. Base excess and base deficit refer to an increase or decrease, respectively, in total buffer base. In acute respiratory acidosis, total buffer base does not change because the accumulation of HCO3- is accompanied by an equivalent decrease in the concentration of other buffers, such as Hb. Therefore, there is no base excess or base deficit.
The ideal way to correct respiratory acidosis is to restore alveolar ventilation. However, because disease processes that impede ventilation cause the respiratory acidosis, this option is not available to the animal, and other means to correct pH, primarily renal mechanisms, must be used. The elevated Pco2 and decreased pH increase H* and NH3 production in the kidney. This increases the elimination of H- in the urine and generates new HCO3-, and as the plasma [HCO3-] increases,
the ∣HC0370.03 ∙ Pco2] ratio and pH are adjusted toward normal. The newly generated HCO3 adds to the total buffer base and therefore causes a base excess. Figure 52-4 shows how this accumulating HCO3" adjusts the pH toward normal during respiratory acidosis, even though Pco2 remains constant.