Steroid Hormones and Other Lipid Signals Interact with Nuclear Receptors, Which Are Transcription FactorsWithin the Cell
Nuclear receptors are another large class of protein molecules specialized for information transmission and transduction. Nuclear receptors are sufficiently numerous and diverse that they compose a “superfamily” of evolutionarily conserved and related receptors, as with the GPCRs.
All nuclear receptors are transcription factors that respond to the binding of their cognate lipid signal by regulating which genes are expressed within particular cells under particular conditions. Accordingly, one of the conserved features of nuclear receptors is their DNA-binding domain, which can bind directly to specific sequences of DNA (promoter regions) that control the expression of the neighboring gene(s) (Figure 1-20). As with all other proteins, the DNA binding function of nuclear receptors is based on their shape. The DNA-binding domain, for example, is a part of the protein shaped into “fingers” by a zinc ion. These zinc fingers, also found in many other transcription factors, fit into the grooves of the double helix of DNA at the appropriate base-pair sequence.Recall that steroid hormones are soluble in oily solvents and are able to diffuse through the lipid bilayer without the mediation of transport proteins. Thyroid hormones are also lipophilic and diffuse through the lipid bilayer. Additionally, several lipid-soluble nutrients are also signaling molecules, including vitamins A and D. Vitamin A is required for vision because it is the covalently bound cofactor for the opsin GPCRs, but it also plays a role in embryonic development. Vitamin D controls Ca2* metabolism. Similarly, saturated and unsaturated fats in the diet are also known to provide signals that control their own breakdown and metabolism and to regulate the differentiation of fat cells (adipose tissue). Consequently, the receptors for these lipid signals are soluble proteins within the target cell.
'Γhe cellular location of the nuclear receptors varies. Some receptors can be found in the cytoplasm before ligand binding, whereas others are largely restricted to the nucleus (after their initial synthesis in the cytoplasm), but all are functional as transcription factors in the nucleus after activation. The lipid-soluble hormone/nutrient diffuses from the blood into the cell and binds to its receptor, and the hormone/receptor complex is, as in previous examples, the physiologically active entity that ultimately triggers a cellular response. As noted earlier, because the nuclear receptor complex is itself a transcription factor, steroid and thyroid hormones do not require a second messenger; the hormone/receptor complex is itself active within the cell, altering gene expression.A well-studied example of nuclear receptor action as a regulated transcription factor, with some relevance to veterinary medicine, is the action of estrogen on the reproductive tracts of female chickens (see Figure 1-20). Estrogen is the principal female sex hormone of birds and mammals, and, of course, hens lay eggs whose embryo and yolk is surrounded by an “eggwhite.” The principal protein of eggwhite is ovalbumin, which is secreted by the epithelial cells of the avian oviduct as the ovum slides by. Thus, one of estrogen s targets in female chickens is oviduct epithelial cells. Estrogen enters the cytoplasm of these cells and binds to its receptor, the estrogen receptor. 'Fhe hormone/receptor complex, but not the ligand- free receptor, is able to mediate estrogen-specific, essentially female-specific, gene transcription. The estrogen receptor complex binds to a sequence of DNA, called an estrogen response element, that controls the transcription of a neighboring gene, for ovalbumin in this case. In other cells of the female, binding of the estrogen receptor to the estrogen response elements of other genes would cause these other female-specific genes to be transcribed and ultimately expressed as a protein (e.g., proteins in yolk of egg).
Different steroids bind to different receptors (e.g., male sex hormone testosterone binds to testosterone receptor), which bind to different response elements, leading to different genes expressed (e.g., male-specific gene expression).Differential gene expression and its regulation were initially pursued primarily by molecular biologists. It rapidly gained importance in physiology, however, and will do so soon in veterinary medicine. Humankind will have fewer scruples about controlling gene expression in domestic animals than lor their own species. Indeed, understanding control of gene expression may prove more important to veterinary students in the near term than for students of human medicine.
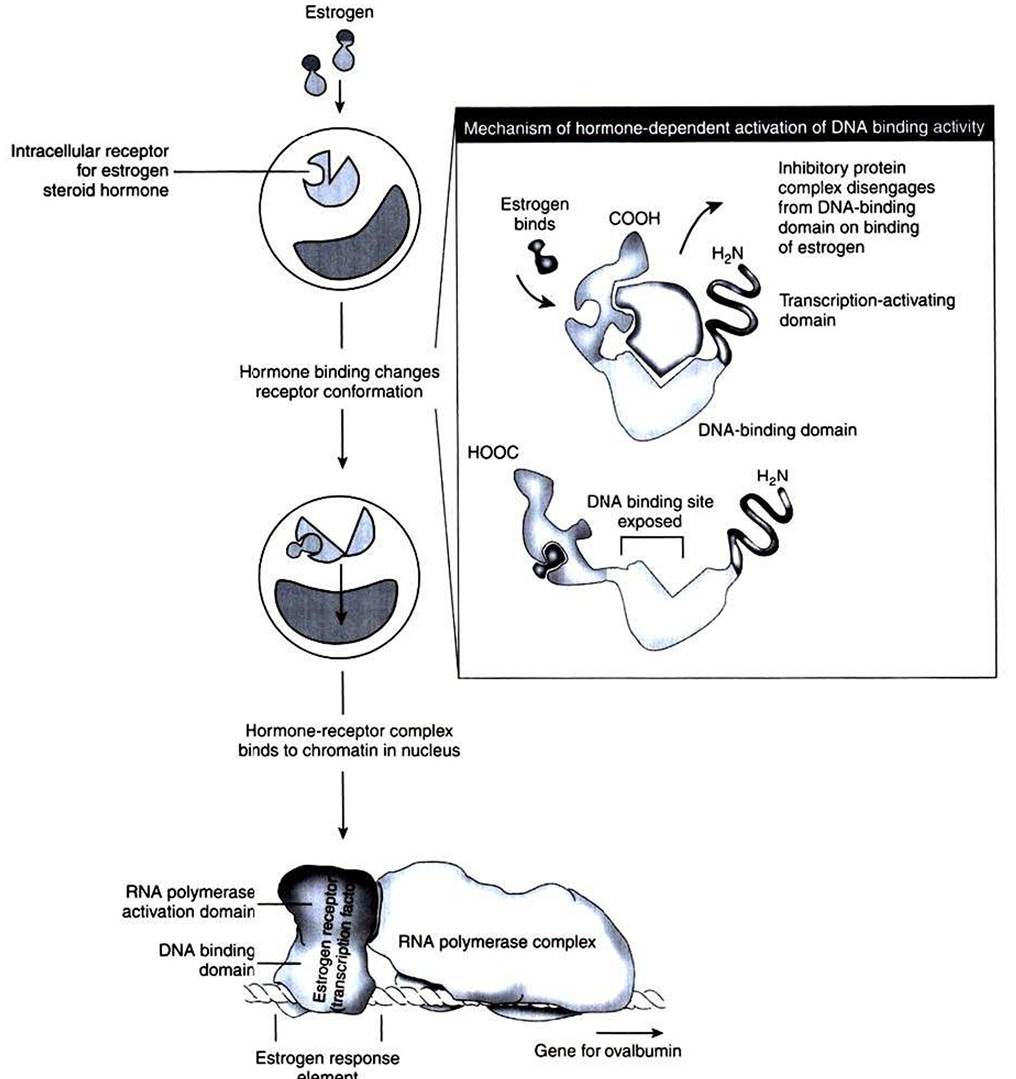
FIGURE 1-20 Steroid hormone action as illustrated by control of ovalbumin expression by estrogen in hens. The steroid hormone estrogen penetrates the lipid bilayer passively because of the oil solubility of the steroid. Inside the cell, the estrogen binds to a cytoplasmic receptor, the estrogen receptor.The binding of estrogen to its receptor causes the receptor protein to change conformation, which in turn changes the DNA-binding activity of the receptor. The hormone/receptor complex enters the nucleus and binds to regulatory sequences of DNA, the estrogen response element.This binding, in turn, activates ribonucleic acid (RNA) polymerase. This initiates transcription of the ovalbumin gene, an estrogen-responsive gene, to produce messenger RNA (mRNA), which is ultimately translated into the ovalbumin protein for secretion.
CLINICAL CORRELATIONS
Peripheral Edema
History. You examine a 2-year-old cow that has been grazing on a poor-quality pasture. The owner states that the cow seems to have a poor appetite, walks slowly, and stands apart from the rest of the herd. The cow has developed swelling beneath the skin of her brisket and ventral thorax.
Clinical Examination.
On clinical examination, you find a listless cow standing in a pasture littered with various metal objects. Examination of the cardiovascular system reveals distended jugular veins and abnormal heart sounds characterized by irregular sloshing sounds throughout the cardiac cycle that drastically muffle the first and second heart sounds. Subcutaneous edema (swelling) can be seen throughout the chest and abdomen, but most prominently in the dependent ventral areas of the thorax. Pushing on these swollen areas leaves a dent (pitting edema).Comment. This is a characteristic history of a cow with hardware disease. The cow, grazing on a pasture littered with metal debris, swallows nails, wire, and so forth. Because these objects are heavier than the feed, they drop into the reticulum, a stomach chamber located just caudal to the diaphragm and heart. With the contractions of the reticulum, a metal object migrates through the reticular wall, diaphragm, and pericardium, leading to an inflammatory response in the pericardium (pericarditis). The resulting process is caused by both inflammation and possible secondary bacterial infections from a contaminated metal object traversing regions of the gastrointestinal tract that contain numerous microorganisms, before the object penetrates the pericardium. An inflammatory exudate fills the pericardial sac; it muffles the heart sounds, and a sloshing sound may be heard on auscultation. As this exudative fluid fills the pericardial sac, it limits the pumping efficiency of the heart by limiting its filling during diastole and by obstructing venous return to the heart (see Chapter 21). The result is left-sided heart failure because the heart cannot circulate (pump) the blood throughout the body. This causes the blood to accumulate initially, leading to an increased hydrostatic pressure in the veins and capillaries. As the capillary hydrostatic pressure rises, capillary filtration is favored over reabsorption, and water leaves the capillary and accumulates in the interstitial space. This accumulated interstitial fluid, primarily as the result of increased capillary filtration, is seen clinically as edema. The other common cause of edema is decreased capillary colloidal osmotic pressure from low serum protein. However, this does not usually play a part in hardware disease.
Treatment. Treatment includes surgical removal of the foreign object or objects, antiinflammatory agents, and antibiotic treatment for the pericarditis. Even though considerable inflammation is present, a secondary bacterial infection often contributes to the response. In such an advanced case, however, treatment often is not completely successful.