STUDY OF THE LIVE ANIMAL
Regional anatomy is conveniently studied by dissection, but this has obvious limitations if the goal is knowledge of the anatomy of the living. When embalmed, organs are uncharacteristically inert and greatly changed in color and consistency from their living state.
The impressions gained in the dissection room or from prosection must therefore be modified and corrected by frequent reference to fresh material and by observation of surgical operations, whenever possible. Because most of those who study the anatomy of domestic animals do so with a future professional career in mind, they will find it both stimulating and advantageous to learnhow to apply the simpler methods of clinical examination to normal animals at this stage in their training. Students in some departments receive elementary instruction in these methods; others must create their own opportunities, perhaps by enlisting the assistance of senior student colleagues. They will find a little direct experience to be far more rewarding than much unsupported reading. We merely list some methods and rely on our colleagues in the clinics to provide more adequate guidance.
The simplest method is observation of the contours, the proportions, and the posture of the body. Bony projections provide the clearest landmarks, but superficial muscles and blood vessels are also useful, if less striking; reference to these landmarks allows the positions of other structures to be deduced from their known relationships. Little experience is required to reveal the importance of breed, age, sex, and individual variation or to show that although some landmarks are fixed and reliable, others are prone to move. Some (e.g., the costal arch) move with each respiration, whereas other features change more gradually, for example, becoming more or less prominent or shifting in position with the deposition or depletion of fat or with the advance of pregnancy.
Structures that are not directly visible may be identified by touch, that is, by gentle or firmer palpation as circumstances require. Bones may be identified by their rigidity, muscles by their contraction, arteries by pulsation, veins by swelling when the blood flow is interrupted by pressure, and lymph nodes and internal organs by their size, configuration, and consistency. Nonetheless, variation is great and is affected by many factors that make it difficult to know whether one should expect to be able to identify certain organs in all normal subjects, which is, itself, another useful lesson. Palpation through the skin can be supplemented by digital or manual exploration per rectum and per vaginam.
Certain organs may be identified by percussion to elicit resonance when the overlying skin is struck a sharp blow (in a prescribed fashion). Different materials produce different notes; that from a gas-filled organ is more resonant than the duller one elicited from an organ that is solid or filled with fluid. The normal activities of certain organs produce sounds continuously or intermittently. Although the lungs and heart (not forgetting the fetal heart) are the prime examples of organs whose positions can be determined by auscultation, the movement of blood within vessels or of gas or ingesta within the stomach or intestines can also be a useful source of anatomical information. When these two techniques are applied, it must not be forgotten that the vagaries of sound conduction through materials of different densities may provide a distorted indication of the position and dimensions of the source.
The study of the anatomy of the live animal can be enlarged by other methods whose exercise requires considerable training and more elaborate apparatus than the simple stethoscope. These additional procedures have provided a variety of new illustrations scattered through later chapters but, while some elementary knowledge of how these illustrations were obtained may assist their appreciation, detailed consideration of the various technologies involved is clearly beyond the scope of this book.
Many parts and cavities that are normally out of sight can be brought into view by the use of various instruments. Perhaps the most familiar of these are the ophthalmoscope, used to study the fundus of the eye, and the otoscope, used to explore the external ear canal. Other instruments, for which the generic title “endoscope” is available, may be introduced into natural orifices and advanced to allow inspection of deeper parts, such as the nasal cavity, bronchial tree, or gastric lumen. These examples of endoscopy are noninvasive, but other examinations require preparatory surgery. Among these are arthroscopy, the inspection of the interior of synovial joints, and laparoscopy, the technique in which an endoscope is passed into the peritoneal cavity through a small opening in the abdominal wall. This last technique may be employed for diagnostic purposes or for the visual control of (“keyhole”) surgery with the use of instruments introduced through separate portals. For both purposes, moderate inflation of the abdomen creates the necessary viewing chamber.
Early endoscopes were rigid, which limited their utility, but the modern fiber-optic version is flexible and can negotiate bends while its tip may be turned, under remote control, to widen the field that may be scrutinized. The essential components of the fiberoptic instrument are two bundles of glass fibers. Such fibers, when suitably prepared and coated, conduct light from one end to the other without significant leakage to the side. One bundle is used to convey light distally, from an external source to the region to be viewed; the component fibers can be relatively coarse and randomly arranged. The second bundle conveys the image and is composed of finer fibers that maintain fixed positions in relation to each other. The image is composed of many tiny units, each corresponding to an individual fiber, and is presented to the eye (or to a camera or video system) at the proximal end of the instrument.
Radiographic anatomy has for some time been an indispensable component of every course of anatomy influenced by clinical considerations.
Most departments routinely display previously prepared radiographs and, although students are unlikely to be involved in their production, it is prudent to remind them that considerable risks are associated with x-radiation—risks that must always be assessed for those conducting and those subjected to these procedures.X rays are produced by bombarding with electrons a tungsten target (focus) housed within a shielded tube. Only a narrow x-ray beam is permitted to escape, and this is directed toward the relevant region of the subject. The passage of the rays through the body is affected by the tissues they encounter; tissues substantially composed of elements of high atomic weight tend to scatter or absorb the rays; tissues substantially composed of elements of low atomic weight have proportionately less effect. Because of its calcium content, bone clearly belongs to the first (radiopaque) category, whereas soft tissues generally belong to the second (radiolucent) category. Those rays that succeed in passing through the subject are allowed to impinge on a sensitive film (or other detector), which responds to the radiation received. When the film is developed, those areas that were overlain by soft tissues (or gas-filled spaces) appear dark, even black, while those areas that were overlain by bone (or other radiopaque material) appear lighter, even white. The distinction between tissues of similar radiodensity may be enhanced by introducing an appropriate contrast agent to coat a surface or fill a space. Specific methods, utilizing various materials, are available to depict such different features as the gastric lumen, urinary tract, and subarachnoid space.
Radiographic views are appropriately identified by reference to the direction taken by the x-ray beam in its passage through the subject. Thus a radiograph of a supine animal, presenting its belly toward the x-ray source, is described as a ventrodorsal film; that obtained with the animal turned over, with its belly now facing the film, is described as a dorsoventral film.
The convention provides little scope for confusion but occasionally produces an awkward term, such as dorsolateral- plantaromedial which specifies a particular, oblique view of the hock.Awareness of certain general principles will help in the avoidance of some common misinterpretations: the image of any structure is always magnified to the degree determined by the ratio focus-film/focus-object; the divergence of the x rays produces an apparent shift in position of any object not directly below the focus. Two simple diagrams (Figure 1-2) will make these points clear. A less easily resolved difficulty results from the superimposition of the images of structures that lie over each other. An ingenious, only partly successful, solution to this problem was sought in the coordinated movement—in opposite directions—of tube and film during the period of the exposure (Figure 1-3, A). In this technique, known as tomography, the axis about which tube and film travel coincides with the plane of the horizontal slice of the subject that is of current interest. Structures contained within this slice remain more or less in focus throughout the exposure, while the images produced by structures at other levels are blurred or subsumed within the general background. Such tomograms never found much employment in veterinary radiology. The more recently developed and more sophisticated technique known as computed tomography (CT) has a different basis but retains the aim of clearly depicting the parts within one particular body slice while excluding extraneous images. Despite the considerable cost of the apparatus and its limited suitability for use with large animals, the technique is now widely offered by veterinary referral centers.
In the modern CT scanner, the x-ray source is moved in a circle that is centered on the longitudinal axis of the subject during the procedure, which takes from one to several seconds for its completion (see Figure 1-3, B). During this time the movement of the tube is repeatedly arrested for very short periods; during each of these, a burst of radiation is directed through the subject along a different radius.
The beams that penetrate the selected, very narrow slice of the subject impinge on a series of discrete detectors or, in some designs, on portions of a continuous circumferential detector and are photomultiplied. After the procedure is completed, these records are analyzed, compared, and combined according to complex formulae (algorithms); from these computations, a single cross-sectional image is constructed in which the forms, locations, and comparative radiodensities of all the tissues within the selected body slice are represented (Figure 1-4). In more complex settings, multiple overlapping or adjacent slices can be imaged in an extended, continuous process. With the amount of information the extended process supplies, it is possible by even more elaborate computation to construct images in other than transverse planes. The data may also be manipulated to enhance subtle differences in contrast presented by tissues of very similar radiodensity.CT is, of course, not free from all drawbacks: subjects must be strictly immobilized during the exposure procedure; the total radiation dose may be quite considerable, even though individual exposures are very short and the resulting images amplified; artifacts may produce deceptive images; current apparatus designed for medical use is suitable for small animals but must be adapted for application with large animals and is then limited to the investigation of the head and limbs. One by-product of CT is the revival of interest in crosssectional anatomy, an approach to the discipline that was, until recently, regarded as irretrievably passe but is now clearly indispensable for CT interpretation.
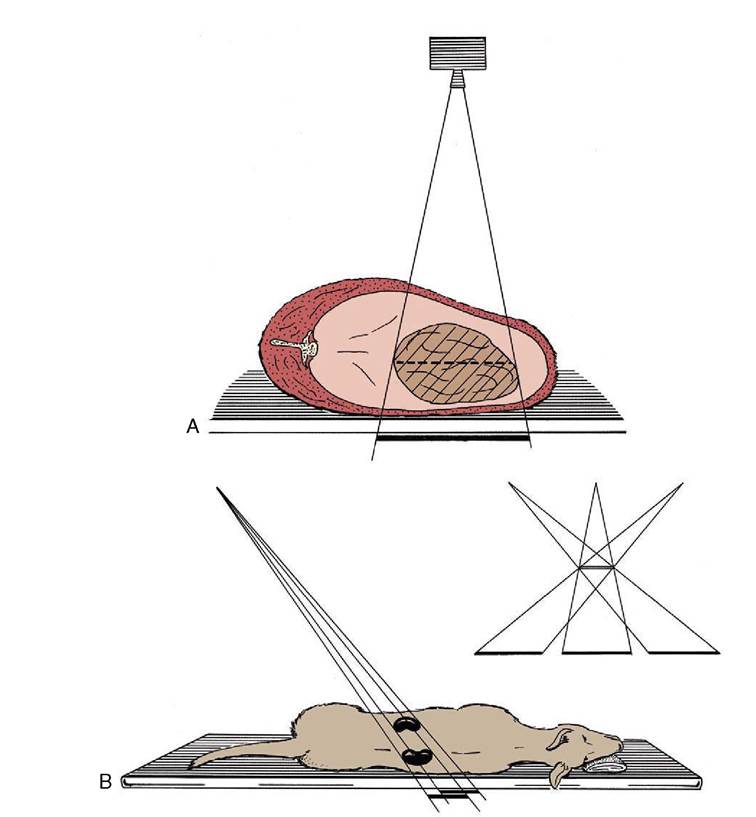
Figure 1-2 A, Schematic drawing illustrating the magnifying effect caused by the divergence of the x rays. B, Schematic drawing illustrating the apparent shift in position of an organ that is not directly below the focus.
Familiarity with cross-sectional anatomy is also required for the practice of ultrasonography. This technique depends on the capacity of a piezoelectric crystal to convert electrical energy into sound waves and vice versa. When stimulated, a suitably housed crystal transducer, coupled to the appropriate area of skin, directs a narrow beam of sound waves of uniform frequency into the body. The waves are propagated through the tissues with decaying intensity, and a fraction is directed back toward the source at each encounter with an interface between tissues offering different resistance (acoustical impedance). Reconverted into electrical energy, the echoes generate a visible image on a screen. This image, which can be “frozen” or recorded in various ways, represents the thin body slice directly below the transducer. The sound wave is not produced continuously but in very short bursts, perhaps lasting for no more than one-millionth part of a second. The longer silences that alternate with these bursts allow the time necessary for the receipt of echoes bounced back from interfaces at different depths.
The frequency and the wavelength of sound waves are inversely related. The first variable determines the depth to which waves will penetrate, the second, the resolution that may be obtained (i.e., the detail that may be distinguished). Because waves of high frequency penetrate less deeply but record more detail, a compromise is involved in the selection of the appropriate crystal to deploy for a specific examination: several crystals are normally at hand, and each has its own inherent and invariable oscillation frequency. The maximum depth from which it is possible to obtain useful images is about
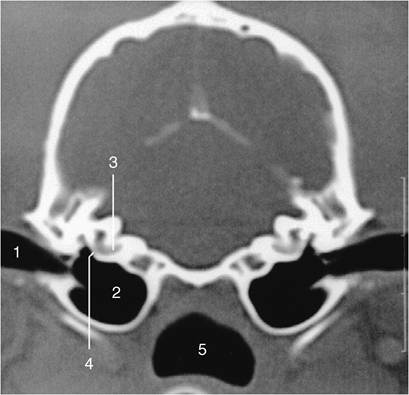
Figure 1-4 Transverse image of a 2-mm-thick computed tomographic slice of the canine tympanic bullae and petrous temporal bones. (Bone settings were used.) 1, External acoustic meatus; 2, tympanic bulla; 3, cochlea; 4, round window; 5, nasopharynx.

Figure 1-3 Diagrams of a basic (noncomputed) x-ray tomographic apparatus (A), and of a fourth-generation computed tomographic (CT) scanner (B). 1, Movement of x-ray source during exposure; 2, lines indicating mechanical connection between x-ray source and radiation detector (i.e., film); 3, plane of focus; 4, supine patient on stationary table; 5, movement (in the opposite direction) of detector during exposure; 6, movement of x-ray source around stationary patient; 7, x-ray beam during exposure; 8, ring of fixed detectors surrounding the rotating x-ray tube mechanism.
25 cm, and this limits the application of ultrasonography in horses and cattle. In these large species its use is more or less restricted to the examination of the distal parts of the limbs and of the genital apparatus (when the transducer may be applied to the rectal mucosa). Ultrasonography is also widely used in the diagnosis of pregnancy in sows (although here a transabdominal approach is employed).
Water, blood, and most soft tissues offer very similar acoustical impedance, and interfaces between these substances are, at best, only moderately reflective; they are hypoechoic in Ultrasonographers' jargon. In contrast, the difference in impedance between soft tissue and bone, or between soft tissue and a gas-filled cavity, is very large, and the reflection of sound waves is almost total; the interface is hyperechoic. This makes it impossible to image tissues and organs that, like the brain within the skull, lie deep to bone; such parts are said to be within acoustical shadow. Conversely, a distended bladder, or other large volume of uniform impedance, may be used as a window through which deeper structures may be approached.
There are many differences in transducer design and usage. Some transducers contain multiple crystals arranged in line; when these are activated sequentially, the resulting image is rectangular and represents the thin slice of tissue situated deep to the transducer. More often a single crystal is employed but so arranged that the narrow beam that it generates swings repetitively in an arc, producing a wedge- or sector-shaped image (Figure 1-5). In these B (or brightness) settings, the image represents a cross section through the field surveyed. In the alternative M (or motion) setting, the beam is only emitted at one fixed point in the crystal's oscillation, and the recording is therefore limited to the structures penetrated along a single axis. If the parts are
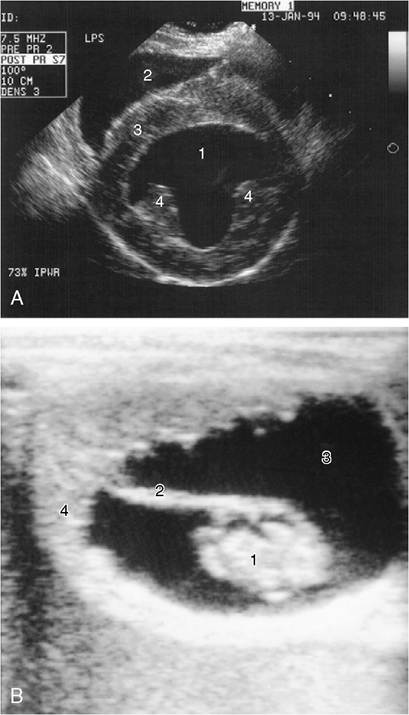
Figure 1-5 A, Ultrasonographic transverse (short-axis) view of the canine heart. 1, Left ventricle; 2, right ventricle; 3, septum; 4, papillary muscles. B, Ultrasonographic view of a 42-day-old equine embryo. 1, Embryo, about 2 cm in length; 2, umbilical cord; 3, allantoic fluid; 4, uterine wall.
moving, successive images reveal their changing shapes, and the changes are emphasized if successive images are recorded side by side. M-mode recordings are especially useful for demonstrating the movements of the walls of the heart chambers and valves.
Ultrasonograms are, in general, less easy for the novice to interpret than radiographs. Reverberations occur when the waves bounce back and forth, often because of defective coupling of the transducer to the skin, and this may produce what appear to be multiple parallel interfaces within an organ. Small interfaces between the parenchyma and fibrous scaffolding of certain tissues produce diffuse scattering, or a stippled effect. Despite these (and other) drawbacks, ultrasonography possesses very considerable advantages, not the least being its freedom from the risks inescapably associated with ionizing radiation.
Magnetic resonance imaging (MRI) requires less extensive consideration because the expenses of the installation and operation of the equipment make it presently available in only a few veterinary centers. The theoretical basis of MRI lies in changes in the structure of hydrogen atoms induced by strong magnetic fields and radio waves. Weak radio signals are subsequently produced when the subatomic structure returns to its normal configuration. These signals may be amplified, and their origins within the body may be precisely fixed in three dimensions. Because different tissues contain different concentrations of hydrogen atoms, their different responses can be used for their distinction. Tissues such as fat that are rich in hydrogen produce bright images in contrast to the black images of hydrogenpoor tissues such as bone (Figure 1-6). Extremely high resolution is possible. There appear to be no health risks associated with the MRI scanner. Both CT and MRI are especially useful in the study of intracranial structures.
SKIN
The skin covers the body and protects it against injury; it plays an important part in temperature control and enables the animal to respond to various external stimuli by virtue of its many nerve endings. There are numerous local modifications of skin (Chapter 10), but at present, we are concerned only with its more general properties.
The skin varies greatly in thickness and flexibility, both among species and locally. It is naturally thicker in larger animals (though not in constant proportion to their size) and in more exposed areas; these inequalities are obviously important to the surgeon. Although the skin is generally closely molded to the underlying structures, it appears redundant in some areas, forming folds and creases; some folding allows for change in posture, some is an adaptation to increase the area through which heat may be dissipated to the environment, and some is no more than the expression of breeders’ whims, grotesquely illustrated by the Shar-Pei breed of dog.
Skin consists of two layers, an outer epidermis and an inner dermis, and in most situations it rests on a looser connective tissue variously known as the subcutis, hypodermis, or superficial fascia (Figure 1-7). The epidermis is a stratified squamous epithelium whose thickness is adapted to the treatment it receives; it responds to rough usage, as exemplified by the footpads of dogs and cats. Numerous modifications of this layer exist, the most common being the occurrence of sweat and sebaceous glands and of hair. Sweat glands are most important as a provision for heat loss by surface evaporation but also play a subsidiary role in the excretion of waste. The sebaceous glands produce an
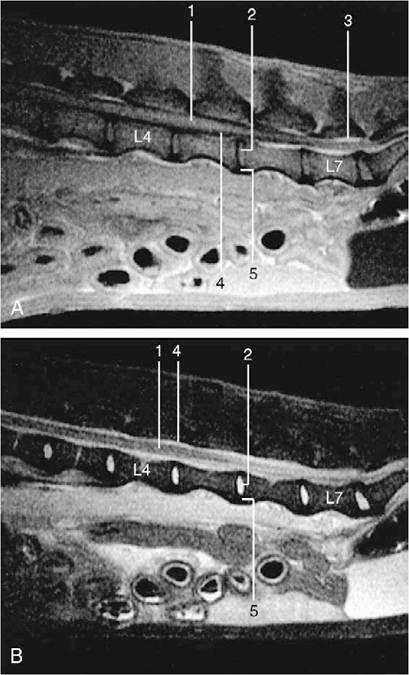
Figure 1-6 Midsagittal images of 3-mm-thick spin-echo magnetic resonance slices of the canine lumbar vertebral column. A, Tl-weighted (fat appears white, fluids dark). B, T2-weighted (fluids appear white, fat darker than on Tl- weighted images). 1, Spinal cord; 2, nucleus pulposus; 3, epidural fat; 4, cerebrospinal fluid; 5, annulus fibrosus.
oily secretion that waterproofs the surface and provides certain relatively naked areas, such as the groin of horses, with a characteristic sheen. Both types of gland are usually widely, though not ubiquitously, spread. The haircoat, which is a uniquely mammalian feature, is a mechanical protection and a thermal insulator, the latter property depending on the entrapment of air within the pile. The haircoat is also usually widespread. Among the more familiar species, only the human and the pig are relatively naked, although naked individuals may appear in other species as occasional “sports,” which is the origin, for example, of the Sphynx breed of cat. Some aquatic mammals, such as whales, are wholly naked.
The dermis, which consists essentially of felted connective tissue fibers, is the raw material of leather. It is secured to the epidermis by interlocking papillae, which are most pronounced where normal wear might risk
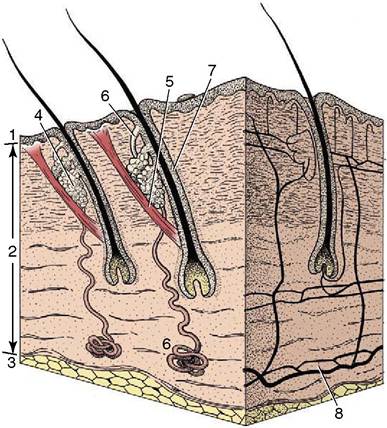
Figure 1-7 A block of skin. 1, Epidermis; 2, dermis; 3, subcutis; 4, sebaceous gland; 5, arrector pili muscle; 6, sweat gland; 7, hair follicle; 8, arterial networks.
separation. In most situations, the skin moves easily over the underlying tissues, and this looseness facilitates the flaying of a carcass. It is more tightly bound down in a few places where it grades into a tougher-than- usual underlying fascia; good examples of this binding are provided by the scrotum and the lips. Some risk of pressure injury is present where the dermis is molded over bony prominences, and synovial bursae (p. 24) often develop adventitiously in such sites. Unlike the epidermis, the dermis is well supplied with blood vessels (see Figure 1-7) and cutaneous nerves.
The superficial fascia is considered in the following section.