Superficial Nerves
Only a few features of the superficial nerves require notice. The facial nerve detaches its auriculopalpebral branch before it enters the face (see Fig. 18.36/24). This branch then takes an independent course across the zygomatic arch (where it is palpable), which leads it between the eye and the ear.
The branch may be blocked by injection between the caudal end of the arch and the base of the ear to facilitate eye examination because it eliminates blinking and closure of the lids (p. 331).The facial trunk divides into dorsal and ventral buccal branches before or, more commonly, shortly after emerging from under the protection of the parotid gland (Fig. 18.7/9). These branches and the smaller divisions into which they soon assort run forward over the masseter, where they are palpable and sometimes even visible through the skin. Blows over the masseter or pressure in prolonged recumbency may damage some or all of the divisions. The asymmetry of the face that results when the muscles of the lips, cheek, and nose are paralyzed is usually more striking than in other species. Because the auriculopalpebral branch is detached proximally, such trauma generally spares the muscles of the eyelids and external ear; their involvement points to injury at a more proximal level, which suggests a more sinister causation (Fig. 18.9).
The trigeminal nerve and its principal branches—the supraorbital, infraorbital, and mental nerves —provide sensory innervation of the face (Table 18.1). These are easily located at their emergence from the corresponding foramina. The supraorbital nerve to the upper eyelid and the adjacent part of the forehead skin leaves the supraorbital foramen within an easily located dimple in the root of the zygomatic process of the frontal bone. Directions for location of the infraorbital and mental nerves have already been given (p. 495). Anesthetic deposited about the infraorbital nerve at its emergence will desensitize the skin of the upper lip, nostril, and much of the nose extending well caudal to the foramen. Blockage of the mental nerve desensitizes the skin of the lower lip and chin region. During blockage of either of these nerves, it is possible to insert the tip of the needle through the foramen into the bony canal within the jaw to desensitize the more rostral teeth (from P2 forward).
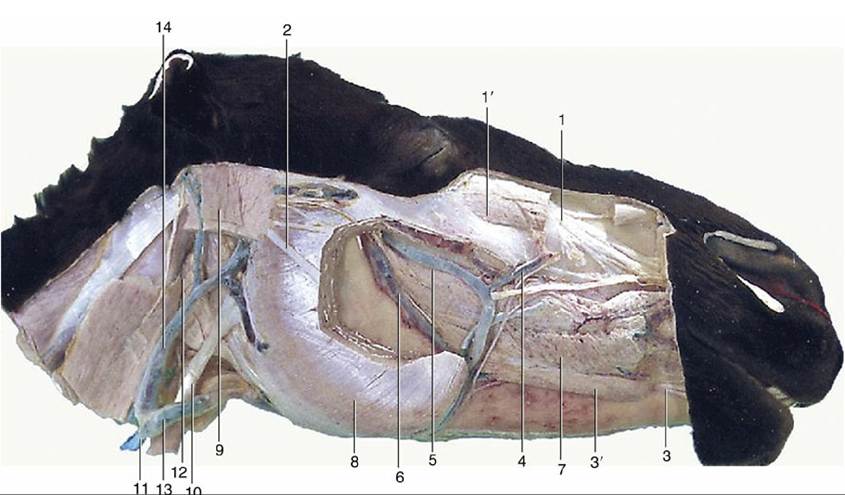
FIG. 18.8 Deeper dissection of the head. Parts of the superficial muscles, masseter, and parotid gland have been removed. 1, Infraorbital nerve; 1', levator labii superioris; 2, dorsal buccal branch of facial nerve; 3, mental nerve; 3', depressor labii inferioris; 4, facial vein; 5, deep facial vein; 6, buccal vein; 7, buccinator; 8, masseter; 9, occipitomandibularis; 10, sternocephalicus; 11, external jugular vein; 12, mandibular gland; 13, linguofacial vein; 14, maxillary vein.