THE ABDOMINAL CAVITY
Some general observations concerning the abdominal cavity are necessary before continuing the description of the digestive system.
The abdomen is the portion of the trunk that lies caudal to the diaphragm (p.
32). It contains the largest of the body cavities, which is continuous at a plane passing through the sacral promontory and the pubic brim with the more caudal and very much smaller pelvic cavity (see Figure 2-2). The more cranial (intrathoracic) part of the abdominal cavity is protected by the hindmost ribs and costal cartilages and is rather restricted in the variations in size that it may experience; the more caudal part is supported by the skeleton only on its dorsal aspect and is therefore more variable. The pelvic cavity has the most extensive bony support and the most constant size, although even here a certain latitude is allowed by changes in the soft tissue components of its walls (see Figure 29-25, A-B).The structure of the abdominal and pelvic walls has been described with the locomotor apparatus. Comparative features, including conformation and the factors that influence this in different species, are considered in later chapters. The abdominal and pelvic cavities contain the peritoneal sac; the stomach, small and large intestines, and associated liver and pancreas; the spleen; the kidneys, ureters, bladder, and urethra (in part); the ovaries and most of the reproductive system in the female and a smaller part of the reproductive tract in the male; the adrenal glands; and many nerves, blood vessels, and lymph nodes and vessels.
Peritoneal structures
An incision through the whole thickness of the abdominal wall enters the peritoneal cavity, which is a division of the celom that is bounded by a delicate serous membrane, the peritoneum. The peritoneal cavity is completely enclosed in the male, but in the female a potential communication with the exterior exists at the abdominal opening of each uterine tube.
The peritoneal cavity contains only a small amount of serous fluid because the abdominal organs are excluded from the space by their peritoneal covering. Nonetheless, it is common to designate as intraperitoneal those organs that are suspended from the abdominal roof within the peritoneal reflections. Although misleading, the term is useful in emphasizing the difference between this and the alternative retroperitoneal arrangement of other organs that are directly joined to the abdominal wall. A diagram (Figure 3-32) may make the distinction plain. The same diagram illustrates the division of the peritoneum into a parietal part lining the walls (parietes), a visceral part directly enshrouding the organs (viscera), and a series of double folds connecting the parietal to the visceral parts. These folds are often collectively known as mesenteries, but properly this term is restricted to the fold suspending the small intestine (and more specifically only the jejunum and ileum); certain similar folds are conveniently named mesocolon, mesovarium, and so on, according to the organ that they support. Others, for example, the greater omentum, have names less immediately revealing.A small outpouching (infracardiac bursa) of the parietal peritoneum extends a little way into the mediastinum within the thorax along the right face of the esophagus where this penetrates the diaphragm.
The peritoneum consists of a single layer of flattened mesothelial cells supported by a fibroelastic tissue that attaches, more or less firmly according to position, to the underlying structures. A considerable amount of fat is often stored below the peritoneum, and some locations are especially favored. In the healthy animal the peritoneal cavity is reduced to a series of clefts between
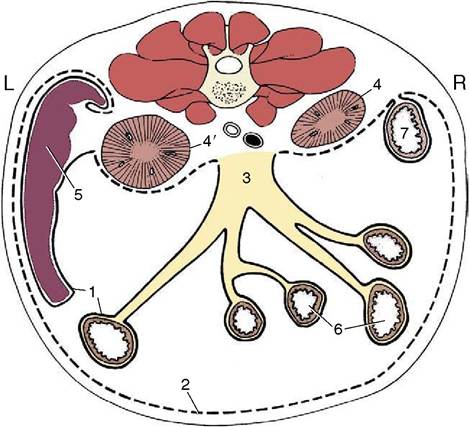
Figure 3-32 Schematic transverse section through the abdomen of the dog. 1, Visceral peritoneum (continuous line); 2, parietal peritoneum (broken line); 3, root of mesentery; 4, 4', right and left kidneys (retroperitoneal); 5, spleen; 6, jejunum; 7, descending duodenum.
the closely packed abdominal organs. Most clefts are of capillary dimensions, and the total volume of the peritoneal fluid is therefore small—a few milliliters in the dog. The fluid is nonetheless of vital importance, for it lubricates the viscera, allowing them to slip freely over each other or against the abdominal wall in the performance of their own functions or when displaced by other activities. The fluid is constantly turned over, although the mechanism of resorption is disputed. Whatever its nature, the large surface area (2 m2 in humans) of the peritoneum aids rapid removal, and drugs are sometimes administered by intraperitoneal injection. Toxins are also readily absorbed, and because the warm and moist peritoneal cavity affords ideal conditions for bacterial growth, inflammation of the peritoneum is never regarded lightly.
Inflamed serous sheets have a tendency to stick together, and in the course of time these adhesions may become organized and permanent. For this reason the surgeon often turns in the edges of the wound, bringing serosal surfaces together, when closing an incision. Adhesion between organs that are normally free to move over each other is a possible and undesirable sequel to infection or trauma of the peritoneum. Clearly, any attachment that limits mobility may interfere with normal function. However, it must also be noted that adhesion of apposed serosal surfaces (with the obliteration of the intervening space) is commonplace in development and explains the definitive position and arrangement of many organs and mesenteries.
In early development the gastrointestinal tract pursues a sagittal course through the body cavity. It is attached along its whole length to the roof of the embryonic trunk by a primitive dorsal “mesentery,” but only a portion of the foregut (that which becomes the stomach and first part of the duodenum) and a short caudal portion of the hindgut have similar ventral attachments. The parts of the dorsal mesentery associated with the differentiating organs are assigned appropriate names and may be listed in succession: (dorsal) mesogastrium, mesoduodenum, mesojejunum, mesoileum, mesocolon, and mesorectum.
The ventral connection to the stomach is known as the ventral mesogastrium. The mesojejunum and mesoileum together constitute the (great) mesentery of adult anatomy. Most portions of the dorsal mesentery persist in more or less unmodified form (at least in the dog), but the mesogastria have a more complicated fate dictated by the later development of the stomach.The dorsal mesogastrium becomes drawn out and folded on itself during development and is then known as the greater omentum. The folding creates a pouch, the omental bursa, enclosing a portion of the peritoneal cavity. However, the pouch is flattened and its walls brought into close contact so that the cavity is potential, not actual. The greater omentum of the dog is turned caudally between the viscera and the abdominal floor, and its walls are described as parietal (ventral) and visceral (dorsal) because of their relationship to the abdominal wall and viscera. It is the first structure to appear when the abdominal floor is opened. The later growth of the liver reduces access to the interior of the bursa to a narrow opening known as the epiploic (omental) foramen, through which the cavity of the omental bursa remains in open, if restricted, communication with the major part of the peritoneal cavity. The main features of the arrangement are shown in Figures 3-33 and 3-61. The differential growth and the secondary attachments that determine the adult arrangement vary considerably between species, and those details that possess a practical importance are mentioned in context. In most species the greater omentum is lacelike, which is an effect produced by the deposition of fat in strands along the course of the blood vessels; in ruminants so much fat may be present that the omentum appears to consist entirely of this tissue. The omentum has no intrinsic capacity for movement but is liable to be shifted about the abdomen by the movements of other structures. Because it possesses the common tendency of serous membranes to adhere when inflamed, it is often found attached in regions of infection and helps to wall these off.
The surgeon may stitch the greater omentum over a closed incision of a viscus as extra insurance against leakage.The no less complicated arrangement of peritoneal folds that develops, mainly in the pelvic cavity, in association with the urogenital organs is best described with these organs (p. 184).
Visceral Topography
The general disposition of the viscera is determined by the form of the cavity in which they are retained; their detailed arrangement is influenced by individual features of attachment, motility, and distention. Because the peritoneal cavity is hermetically sealed and most abdominal contents are incompressible, it follows that any change in the position or contours of one organ must be followed by adjustment of the abdominal wall or by a reciprocal change in a neighboring organ. In this way a quite trivial change in one organ may set in motion a chain reaction extending into all parts of the abdomen. The weight of the abdominal contents is considerable, especially in the larger herbivores. They “float” within the serous fluid, and the gravitational forces are opposed by the tension actively and passively developed by the structures of the abdominal wall, by the cranial pull on the diaphragm exerted by the negative pressure within the thorax, and, to a lesser and uncertain extent, by the mesenteries and vessels that support particular organs.
The essence of the situation can be conveyed schematically (Figure 3-34). It is seen that the internal pressure varies at different heights within the abdomen; it is
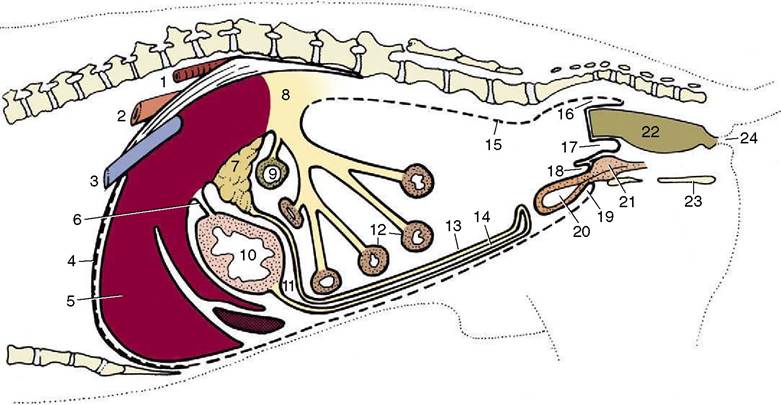
Figure 3-33 Paramedian section of the abdominal cavity of a dog to show the disposition of the peritoneum (schematic). 1, Aorta; 2, esophagus; 3, caudal vena cava; 4, diaphragm; 5, liver; 6, lesser omentum; 7, pancreas; 8, root of mesentery; 9, transverse colon; 10, stomach; 11, omental bursa; 12, small intestine; 13, deep wall of greater omentum; 14, superficial wall of greater omentum; 15, parietal peritoneum; 16, pararectal fossa; 17, rectogenital pouch; 18, vesicogenital pouch; 19, pubovesical pouch; 20, bladder; 21, prostate; 22, rectum; 23, ischium; 24, anus.
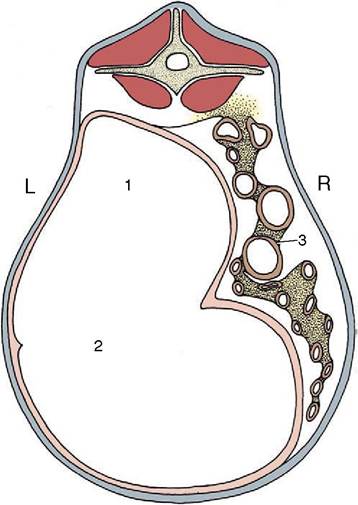
Figure 3-34 Section through the abdomen of a goat. The greater pressure in the lower part of the abdomen causes the convex form of the lower part of the abdominal wall. The pressure within the upper part of the abdomen is below that of the atmosphere, and the flank is sunken. 1, Gas in upper part of rumen; 2, ingesta in the lower part of rumen; 3, intestines.
less than the ambient pressure in the most dorsal part, equal to this at one particular level, and increasingly greater than this toward the abdominal floor. This explains the concavity of the upper part of the flank very evident in cattle and also the tendency for air to rush into the rectum when exploration of this part is clumsily performed. Clearly, the local internal pressures also vary with respiratory changes in intrathoracic pressure and with posture.
The significance of the mesenteries and other attachments in determining visceral topography is disputed. Some of the more robust attachments, for example, those between the liver and the diaphragm, anchor organs quite firmly; others are too frail to play a significant role, and the organs to which they attach must be held in place by mutual contact and by the “lift” of the diaphragm. Certainly, they drop as soon as air is introduced into the peritoneal cavity. The potbellied appearance familiar in many older people is alleged to be in part a consequence of the loss of elasticity in the lungs with resulting reduction of the diaphragmatic “pull.” Some of the arteries that branch from the aorta to supply abdominal organs possess an unusually thick adventitia, and this may allow them to bear some weight when the enclosing mesenteries are fully stretched.
In the dead animal the viscera commonly conform to a fixed pattern. If allowance is made for such obvious factors as the recent consumption of a meal, a tolerably accurate forecast of their disposition can be made before the abdomen is opened, although this introduces air and hence some sagging is inevitable. Therefore, good reason once existed for believing that each of the hollow organs possessed a fairly constant “normal” form. The introduction of radiography destroyed this comfortable illusion, although not before many patients had their organs “tailored” to fit the preconceptions of surgeons reared on traditional anatomy. It can hardly be stressed too strongly that detailed assertions of normal form and position have no place in the description of the hollow organs.
When the positions of the abdominal organs need to be described, it is generally sufficient to relate them to the abdominal wall by means of everyday expressions.