THE BRANCHES OF THE BRACHIAL PLEXUS
With few exceptions, the structures of the forelimb are innervated from the brachial plexus formed by contributions from the last three cervical and first two thoracic nerves (C6-T2).
The plexus reaches the axilla as a broad band that emerges between the parts of the scalenus, but this soon divides into the usual dozen or so trunks. The major trunks, of clinical interest because of their vulnerability to injury or availability for nerve-blocking techniques, are described even though there are few specific features of significance above the carpus.The suprascapular nerve (C6-7) leaves the axilla by sinking between the subscapular and supraspinatus muscles. It then winds around the neck of the scapula before expending itself in the supraspinatus and infraspinatus (Figure 23-43/2). A direct relationship to bone always carries a risk of injury, and the suprascapular nerve may be damaged where it lies against the scapula; apparently this is usually the result of pulling on the nerve as the animal stumbles with the limb stretched back. Injury is therefore most frequent in horses worked over uneven ground. Even serious damage to the nerve may have little immediate effect, although an observer stationed in front of an affected horse may notice a lateral deviation of the shoulder joint at each stride. After a time, muscular atrophy markedly alters the conformation of the shoulder region, causing the scapular spine to project above the wasted muscles. Suprascapular paralysis is commonly known as sweeny or shoulder slip.
The musculocutaneous nerve (C7-8) (Figure 23-43/3,3',3") first runs craniolateral to the axillary artery before turning below the vessel to unite with the median nerve. A branch to the coracobrachialis and biceps is detached before the union. The part incorporated in the median trunk separates in the distal arm and supplies the brachialis and a medial cutaneous antebrachial nerve that crosses the lacertus fibrosus, where it is easily palpated, before being distributed to the skin over the cranial and medial aspects of the forearm and carpus.
Damage to the musculocutaneous nerve cannot be common; however, should such occur, it is unlikely that loss of activity by the principal elbow flexors would greatly affect the gait.The axillary nerve (C7-8) (Figure 23-43/5) has the usual course and distribution—to the principal flexors of the shoulder and the skin over the lateral aspect of the arm and forearm. There appear to be no records of traumatic damage to this nerve in the horse; it is known that in other species section does not impair the gait
because other muscles are potentially able to flex the shoulder.
The radial nerve (C8-T1) is one of the larger branches of the plexus (Figure 23-43/70). It follows the caudal border of the brachial artery in the upper arm and later sinks between the medial and long heads of the triceps, rounding the caudal surface of the humerus to gain the
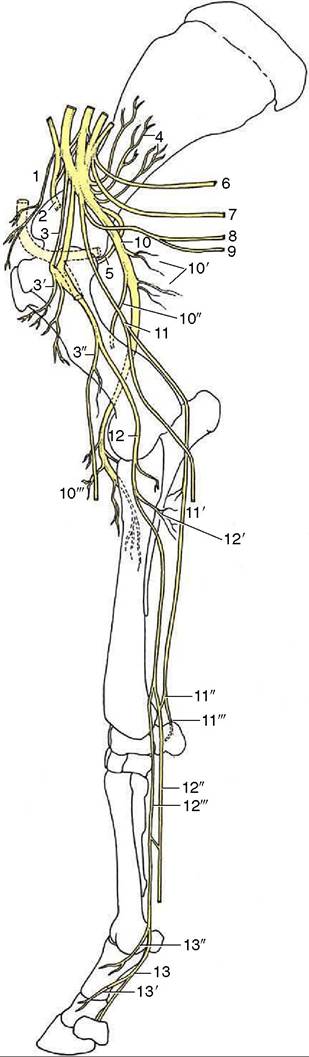
Figure 23-43 Distribution of the nerves in the right forelimb; medial view. The axillary artery at the shoulder joint is stippled. 1, Cranial pectoral nn.; 2, suprascapular n.; 3, musculocutaneous n.; 3', proximal branches; 3", distal branches with medial cutaneous antebrachial n.; 4, subscapular n.; 5, axillary n.; 6, long thoracic n.; 7, thoracodorsal n.; 8, lateral thoracic n.; 9, caudal pectoral nn.; 10, radial n.; 10', proximal muscular branches (triceps); 10", lateral cutaneous antebrachial n.; 10'", distal muscular branches; 11, ulnar n.; 11', caudal cutaneous antebrachial n.; 11", palmar branch; 11'", dorsal branch; 12, median n.; 12', muscular branches; 12", lateral palmar n.; 12’", medial palmar n.; 13, medial palmar digital n.; 13’, 13", dorsal branches.
lateral aspect of the limb. The nerve detaches branches to the triceps group in the proximal part of the arm; more distally, where it is covered by the lateral head of the triceps, it detaches other branches to the extensor muscles of the carpus and digit.
A purely sensory continuation (lateral cutaneous antebrachial nerve) supplies skin over the lateral aspect of the forearm; contrary to the pattern in other species, this branch fades at the carpal level.The radial nerve is the sole supply to the extensor muscles of all joints distal to the shoulder; the effects of damage are therefore proportionately severe. When injury is proximal to the origin of the tricipital branches, the animal is unable to support weight on the affected limb. It stands with the joints uncharacteristically flexed; the angle between scapula and humerus is enlarged, and the elbow is dropped in relation to the trunk. The hoof is rested on its dorsal aspect. High radial paralysis may arise from injury to or disease of the humerus or from damage to the brachial plexus itself. If other components of the plexus are affected, the signs may be complicated by simultaneous paralysis of the flexor muscles of the distal joints.
The results of injury distal to the origin of the tri- cipital branches are naturally less severe. Normal stances of the shoulder and elbow are maintained (Figure 23-46). The animal may rest the dorsal surface of the hoof on the ground but supports weight on the limb if the hoof is first restored to the normal position. Many horses learn to compensate for this disability by setting the hoof down before the impetus—gained when the limb is swung forward during the stride—is lost; the gait may appear almost normal when the terrain is flat, but unevenness quickly brings an affected animal into difficulties. Low radial paralysis may be simulated by the ischemia that sometimes results from prolonged lateral recumbency.
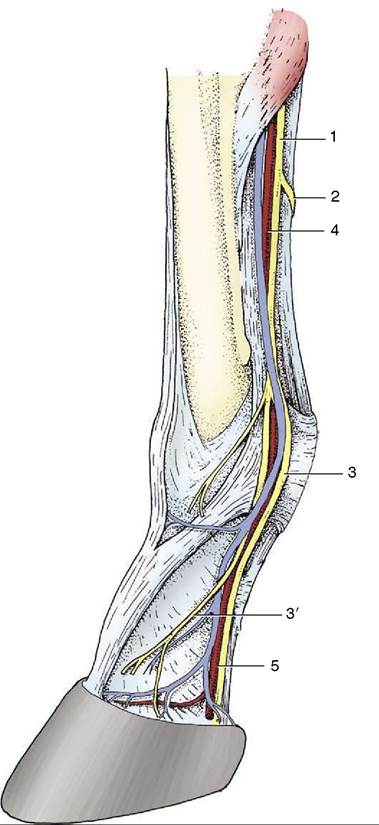
Figure 23-44 Distribution of the medial palmar nerve. 1, Medial palmar n.; 2, communicating branch; 3, medial digital palmar n.; 3', dorsal branch; 4, medial palmar artery and vein; 5, medial digital artery and vein.
The median nerve (C8-T2) is the largest branch of the brachial plexus (Figure 23-46/72). It follows the cranial border of the brachial artery for most of its course through the arm but shifts to the caudal margin on approaching the elbow. It is covered by the pectoralis transversus as it crosses this joint, but even so, the nerve and artery together form a palpable cord (Figure 23-42/7). The two structures continue together as they descend the forearm, buried within the flexor mass of muscle; they divide at the same level, a little above the radiocarpal joint. The end branches, known as the medial and lateral palmar nerves, are described in the next section. The muscular branches to the flexor muscles of the carpus and digit are detached in the very
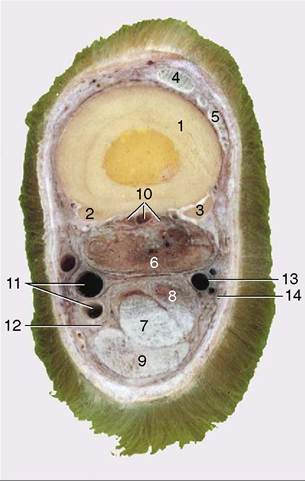
Figure 23-45 Transverse section of the middle of the right metacarpus. 1, 2, 3, Large and small metacarpal bones; 4, common digital extensor; 5, lateral digital extensor; 6, interosseus; 7, deep digital flexor; 8, accessory (check) ligament; 9, superficial digital flexor; 10, palmar metacarpal vessels and nerves; 11, medial palmar artery and vein; 12, medial palmar nerve; 13, lateral palmar artery; 14, lateral palmar nerve.
proximal part of the forearm; beyond these detachments the nerve is purely sensory.
The ulnar nerve (T1-2) follows the caudal border of the brachial artery in the proximal part of the arm (Figure 23-43/77). It then diverges caudally, detaches the caudal cutaneous antebrachial nerve (for the caudal aspect of the forearm), and passes over the medial epicondyle of the humerus before entering the forearm. As it does so, it releases branches to the flexor muscles. The much depleted and now purely sensory nerve follows the ulnar head of the deep flexor at the caudal margin of the limb, under cover of deep fascia (Figure 2341/75). A few centimeters above the carpus it divides into dorsal and palmar branches. The dorsal branch comes to the surface a short distance proximal to the accessory carpal bone and can be palpated against the ulnaris lateralis tendon attaching here; it passes over the lateral aspect of the carpus to expend itself in the skin over the lateral surface of the metacarpus. The palmar branch passes the carpus within the flexor retinaculum, where it exchanges fibers with the lateral palmar nerve, one of the terminal branches of the median.
The overlap of the median and ulnar nerves in their motor distribution makes it unlikely that damage restricted to either one would much affect the gait.
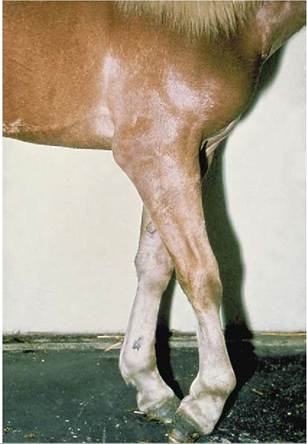
Figure 23-46 Lower radial paralysis.