The Cardiovascular State of Conscious Subjects Is Determined by an Ongoing and Ever-Changing Mixture of Reflex Effects and Psychogenic Responses
The baroreceptor reflex and the atrial volume receptor reflex are only two of several important cardiovascular reflexes. They are primarily responsible for the regulation of blood pressure and blood volume, and they illustrate several properties common to all cardiovascular reflexes.
First, these reflexes originate from changes detected by peripheral sensory receptors. Second, the reflexes occur at a subconscious level, through neural pathways that primarily involve cardiovascular centers in the brainstem and midbrain. Consequently, cardiovascular reflexes persist in unconscious and anesthetized subjects, although the strength and character of the reflexes are altered by anesthesia. Finally, the reflexes use sympathetic and parasympathetic neurons as well as hormonal and behavioral responses to bring about cardiovascular changes.In conscious subjects, neurohumoral control of the cardiovascular system involves both cardiovascular reflexes and psychogenic effects. Psychogenic responses originate from conscious perceptions or emotional reactions. They are eliminated by unconsciousness or general anesthesia. They involve neural pathways of the midbrain and forebrain, including the limbic system and cerebral cortex. Psychogenic responses are often triggered by sensory stimuli. For example, the sights, sounds, and smells of a veterinary clinic may trigger perceptions and emotions that cause increases in heart rate and blood pressure in both animal patients and their human companions. Psychogenic responses can also occur without any obvious sensory triggers. For example, anxiety about a future event can increase heart rate and blood pressure, at least in humans. Cardiovascular reflexes and psychogenic reactions use the same sympathetic and parasympathetic neurons and some of the same hormonal responses to bring about cardiovascular changes.
Two important psychogenic responses are the defense-alarm reaction and vasovagal syncope (the “playing dead” reaction). The defense-alarm reaction (“fear, fight, or flight” response) is an emotional and behavioral response to a threatening situation, physical injury, or trauma. The cardiovascular component of this reaction involves increased sympathetic activity and decreased parasympathetic activity. Typically, the sympathetic activation is sufficiently strong to cause the release of epinephrine and norepinephrine from the adrenal medulla. The cardiovascular responses during a defense-alarm reaction therefore include an increased heart rate, increased stroke volume, vasoconstriction in noncritical organs (kidneys, splanchnic organs, resting skeletal muscle), vasoconstriction in skin, vasodilation in coronary vessels and in working skeletal muscle, and increased blood pressure. The cardiovascular responses during the defense reaction are enhanced by other circulating hormones, including ADH and angiotensin II. The resulting, elevated blood pressure helps to ensure adequate blood flow for the critical organs (exercising skeletal muscles, heart, and brain).
During a defense-alarm reaction, the baroreceptor reflex is reset by the CNS so that it regulates blood pressure at an elevated level rather than acting to oppose the increased pressure. This is analogous to resetting the cruise control on a car so that it regulates speed at an elevated level rather than acting to oppose an increased speed. Thus it is more accurate to say that the baroreceptor reflex regulates blood pressure at a variable set point (set by the CNS) than to say that the baroreflex regulates arterial pressure at any single “normal” pressure.
It is important to recognize that the defense-alarm reaction is simply the extreme form of a continuum of states of emotional arousal. Sleep is at the opposite end of this cardiovascular and emotional continuum. In quiet rest or sleep, sympathetic activity is minimal and parasympathetic activity is maximal.
During a full-blown defense-alarm reaction, sympathetic activity is maximal and parasympathetic activity is minimal. Between these extremes lie all the levels of emotional arousal experienced by animals and humans, from moment to moment, during ordinary and extraordinary daily activities. Cardiovascular variables, such as heart rate and blood pressure, are sensitive to these changes in emotional state (Figure 25-6). For example, a large dog may normally have a heart rate of 70 beats/min while resting at home; it would be entirely normal for the same dog to have a heart rate of 120 beats/min while “resting” in a clinic, if the dog is apprehensive in that setting. Another important point for the clinician to remember is that emotional responses are subjective. Situations that severely agitate one animal may cause only a mild alerting response in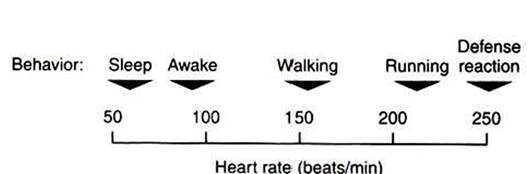
FIGURE 25-6 The defense-alarm reaction is simply the extreme on a continuum of emotional and physical arousal. The cardiovascular system (e.g., heart rate) responds sensitively to every change along this arousal scale.
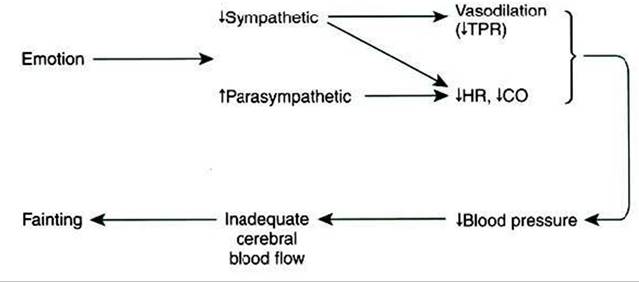
FIGURE 25-7 Vasovagal syncope ("playing dead" reaction) is an emotional response that involves decreases in sympathetic activity and increases in parasympathetic activity. CO, Cardiac output;
HR, heart rate; TPR, total peripheral resistance.
another animal. The clinician must evaluate heart rate, blood pressure, and other cardiovascular signs with respect to the particular patient’s emotional state.
Vasovagal syncope is another psychogenic response that may be encountered in veterinary practice. This response is also called the “playing dead” reaction or ‘playing possum.” In response to certain threatening or emotional situations, some humans and animals experience a psychogenic decrease in blood pressure and may faint.
In many ways, this response is the opposite of the defense-alarm reaction. As shown in Figure 25-7, vasovagal syncope involves a decrease in sympathetic activity and an increase in parasympathetic activity. These neural changes bring about a vasodilation in the noncritical organs and a decrease in TPR. Heart rate and cardiac output also decrease, so there is a large drop in arterial blood pressure. The expected compensatory reflex responses do not take place because emotional state appears to override the baroreceptor reflex in this case. If blood pressure falls so low that there is inadequate cerebral blood flow, the patient faints. The term vasovagal syncope denotes vasodilation, vagal (parasympathetic) activation, and syncope (fainting). It is not clear why some animals respond to a threatening situation with a defense-alarm reaction, whereas others exhibit vasovagal syncope. Also unclear is the survival value of “playing dead,” although this response seems to have served opossums well over several million years.