THE CIRCULATION IN THE FETUS AND THE CHANGES AFTER BIRTH
During fetal life the placenta combines the roles that are later performed by the lungs, the digestive tract, and the kidneys. The blood is therefore replenished with oxygen, provided with nutrients, and cleansed of waste in its circulation through the placenta.
It is returned to the fetus by two large umbilical veins that wind within the umbilical cord and join as one where they enter the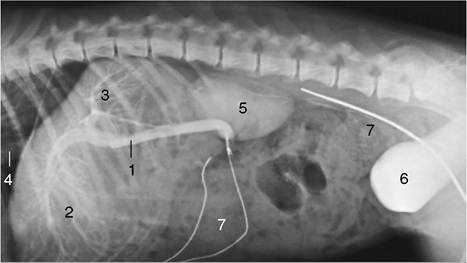
Figure 7-44 Cannulation of the portal vein of a dog. 1, Portal vein; 2, branches to the quadrate, left medial and lateral liver lobes; 3, branches to the remaining liver lobes; 4, caudal vena cava; 5, kidney; 6, bladder, filled with opaque medium; 7, catheters.
body at the navel (Figure 7-45/11). The single intraabdominal umbilical vein runs forward to penetrate the liver at the umbilical fissure before it divides. It detaches collateral branches that vascularize the left portions (umbilical moiety) of the liver while a further branch bends toward the right to make a wide connection with the portal vein (Figure 7-45/12), which vascularizes the right portions (portal moiety). A direct continuation of the umbilical trunk, the ductus venosus (Figure 7-45/9), tunnels through the substance of the liver, bypassing the hepatic circulation, to join the caudal vena cava. The ductus venosus, present in all young embryos, soon becomes vestigial in those of the horse and pig. It persists in other species but varies in caliber and importance and tends to become reduced toward term. The division of the liver into umbilical and portal moieties has obvious functional and possibly also clinical importance. The portal moiety is less generously supplied with oxygen, and this stimulates more active hemopoiesis; the umbilical moiety is more likely to suffer from infections acquired in utero.
The caudal vena cava (Figure 7-45/8) receives the umbilical blood after its passage through the liver and adds it to the deoxygenated blood returned from the hindpart of the body. The oxygen content of the caudal caval stream is therefore already reduced below that of the placental return before it reaches the heart, where the stream impinges on the cranial margin of the foramen ovale (Figure 7-46/2,4). This divides it into two: one part continues into the right atrium (Figure 7-46/5), the other passes through the foramen ovale into the left atrium (Figure 7-46/8). The relative sizes of the two streams change as gestation advances: a continuing shift of the margin of the foramen to the left increases the flow into the right atrium. The right stream mixes with the return from other systemic veins (Figure 7-46/1), and the oxygen content of the blood passed to the right ventricle is thus further diminished. This blood is ejected into the pulmonary trunk (Figure 7-46/6), which in the fetus communicates with the aorta through a wide channel, the ductus arteriosus (Figure 7-46/7'). The ductus enters the aorta beyond the origin of the brachiocephalic trunk and is as wide as the pulmonary trunk (it is in fact its direct continuation—the right and left pulmonary arteries [Figure 7-46/7] are the side branches). The ductus arteriosus receives most of the output of the right ventricle because the vascular bed of the unexpanded lungs offers considerable resistance to blood flow.
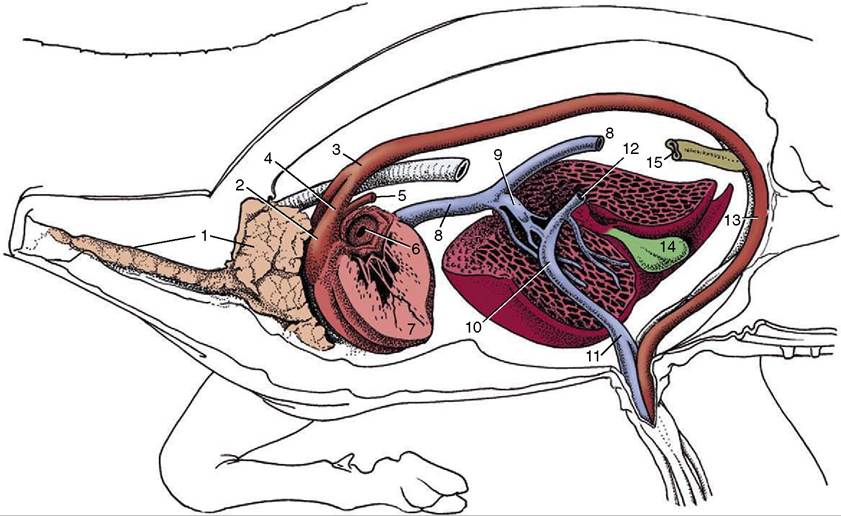
Figure 7-45 Semischematic drawing of fetal circulation (calf). 1,Thymus; 2, pulmonary trunk; 3, aortic arch; 4, ductus arteriosus; 5, pulmonary artery; 6, foramen ovale; 7, wall of left ventricle; 8, caudal vena cava; 9, ductus venosus; 10, junction of umbilical and portal branches within the liver; 11, umbilical vein; 12, stump of portal vein; 13, left umbilical artery; 14, gallbladder; 15, descending colon.
The small flow that is returned to the left atrium from the lungs mixes there with the greater volume of blood that passed through the foramen ovale. The blood that enters the aorta (Figure 7-46/10) is therefore relatively well oxygenated; part of this stream enters the coronary and carotid arteries. The head and brain are therefore favored by receiving a richer supply of oxygen than is given to organs supplied from those branches of the aorta that arise distal to the entry of the ductus arteriosus; these later branches receive the mixed output of both ventricles. The placenta receives the greater share of the flow through the descending aorta (Figure 7-46/10') by way of the umbilical arteries (Figure 7-46/11); these branch from the internal iliac arteries and leave the fetus at the umbilicus, together with the allantoic duct (Figure 7-45/15). The fetal bloodstream is brought into close apposition with the maternal bloodstream within the placenta, although the intervening tissue barrier varies in thickness and permeability among species (p. 209).
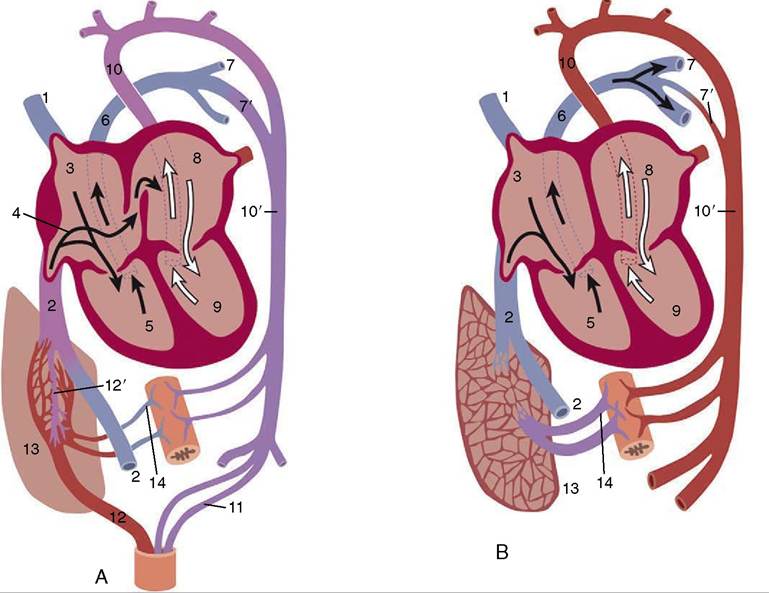
Figure 7-46 Diagrams of the fetal (A) and postnatal (B) circulatory systems. 1, Cranial vena cava; 2, caudal vena cava; 3, right atrium; 4, arrow entering oval foramen; 5, right ventricle; 6, pulmonary trunk; 7, pulmonary artery; 7’, ductus arteriosus (in B, vestige); 8, left atrium; 9, left ventricle; 10, aortic arch; 10', descending aorta; 11, umbilical artery; 12, umbilical vein; 12', ductus venosus; 13, liver; 14, portal vein.
The changes in the circulation that follow birth are not completed as promptly as many believe, and some hours, or even days, may be necessary before a stable circulation of adult pattern is established. The permanent closure of the redundant fetal channels requires a much longer time. The arrest of the placental circulation may precede or follow the initiation of pulmonary ventilation according to the circumstances of parturition.
The umbilical vessels are either bitten across by the mother (e.g., puppy) or are ruptured, being unable to support the weight of the offspring (e.g., calf); in species in which the latter fate is usual, they divide at predetermined levels. In both circumstances little hemorrhaging occurs because the rough treatment stimulates contraction of the muscle in the vessel wall. The arterial stumps are slowly transformed into the round ligaments of the bladder. The stump of the umbilical vein outside the abdomen shrivels, and the intraabdominal part is in time transformed into the round ligament of the liver (p. 436). The raw umbilical surfaces provide potential entry to infection (“navel ill”), and the allantoic duct and thrombosed vein are convenient routes for its spread.The ductus venosus closes within a short time, but how this is achieved and whether closure is to be measured within hours or days are controversial points. Its elimination from the circulation allows the portal vein to perfuse all parts of the liver.
The loss of the umbilical return reduces both the volume and the pressure of the caudal caval stream. This, combined with the concurrent increase in left atrial pressure, halts the shunt through the foramen ovale. Contraction of the muscular wall of the ductus arteriosus is stimulated by the raised oxygen tension of the perfusing blood; it is not effected at once, and for some hours or days blood may shunt in either direction according to the relative pressures in the aorta and pulmonary artery. Expansion of the lungs reduces the resistance of their vascular bed, and the drop in pulmonary arterial pressure results in the flow through the ductus normally being from the aorta. The passage of blood through the constricted tube causes vibration of its wall, which may be detected on auscultation as a continuous murmur during the first day or two of postnatal life in calves and foals. Permanent structural changes eventually obliterate the lumen, converting the duct into a fibrous structure (ligamentum arteriosum); however, for some time after birth the ductus dilates in circumstances that produce hypoxia, and it is often found widely open in the neonatal postmortem specimen.
The increased venous return from the lungs raises the pressure within the left atrium, and this forces the valve of the foramen ovale against the atrial septum, which closes the foramen (Figures 7-25 and 7-46). The valve is a simple flap in carnivores but more elaborate and tubular in ungulates, in which muscle causes it to crumple, improving closure. Although fibrosis eventually seals the valve in place, this takes some time, and it is not uncommon for the opening to be patent to a probe for months or even years; such patency is rarely of significance.
Hypertrophy of the left ventricular wall occurs as a response to the increased workload that is now placed on that chamber. Although little exact information is available on this point for most species, significant relative thickening of the left ventricular wall is already apparent by the end of the first postnatal week in puppies.