The Inguinal Canal
The inguinal canal follows the general pattern but merits a full description because of its relevance to castration, which is performed on the vast majority of male horses. It is the opening in the caudal part of the abdominal wall through which the testis travels in its descent into the scrotum, which is a process usually completed shortly before or shortly after birth in this species.
The canal contains the spermatic cord of the colt and stallion; a stump frequently remains in the gelding. In addition, the external pudendal artery and the genitofemoral nerve travel through the canal.The term inguinal canal suggests a roomier passage, but the canal is no more than a potential space between the flesh of the internal abdominal oblique and the aponeurosis of the external abdominal oblique muscles. The entrance (deep inguinal ring) lies along the free caudal edge of the internal abdominal oblique muscle, which determines its oblique orientation (Fig. 21.4/5); the origin of the internal abdominal oblique from the external abdominal oblique and the convergence of the two muscles on the lateral edge of the prepubic tendon determine its length (generally about 15 cm).
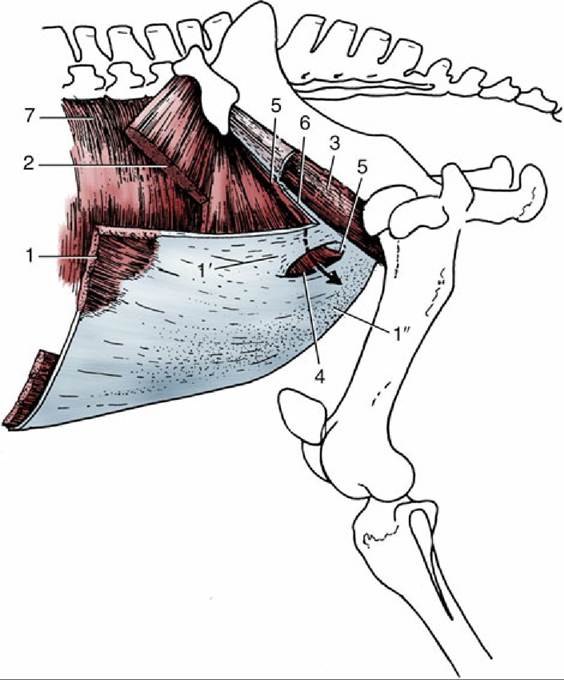
FIG. 21.4 The muscles of the inguinal region. The arrow passes through the inguinal canal. 1, External abdominal oblique; 1' and 1", pelvic and abdominal tendons of external oblique aponeurosis, respectively;
2, internal abdominal oblique; 3, iliopsoas partly enclosed by iliac fascia; 4, superficial inguinal ring; 5, cranial border of deep inguinal ring; 6, attachment of pelvic tendon of external oblique aponeurosis on iliopsoas and sartorius (“inguinal ligament”); 7, transversus abdominis.
The exit (superficial inguinal ring), between the two tendons into which the external oblique aponeurosis splits, is more or less horizontal (Fig.
21.4/4). It is limited laterally by the exchange of fibers between the two tendons where they part company and medially by the tendons meeting and fusing with the edge of the prepubic tendon. The margins of the opening are less clearly defined than many accounts suggest. The lateral (dorsal) crus gives origin to the external spermatic fascia and femoral lamina, which appear to continue the lateral crus directly (Fig. 21.5). The medial (ventral) crus is somewhat frayed but can be identified on palpation through the skin. This is best performed by placing the palm against the belly and advancing the fingers into the cleft between the thigh and abdominal wall. The lateral crus is passed unnoticed, but the medial crus is recognized as a firm edge. The fingers pass into the outer part of the canal most readily with the thigh abducted (when the femoral fascia [lamina] draws the lateral crus outward). It follows from the orientation of the deep and superficial rings that the canal has a triangular outline. It is relatively long cranially and very short caudally where the two openings butt against the prepubic tendon (see Fig. 21.4).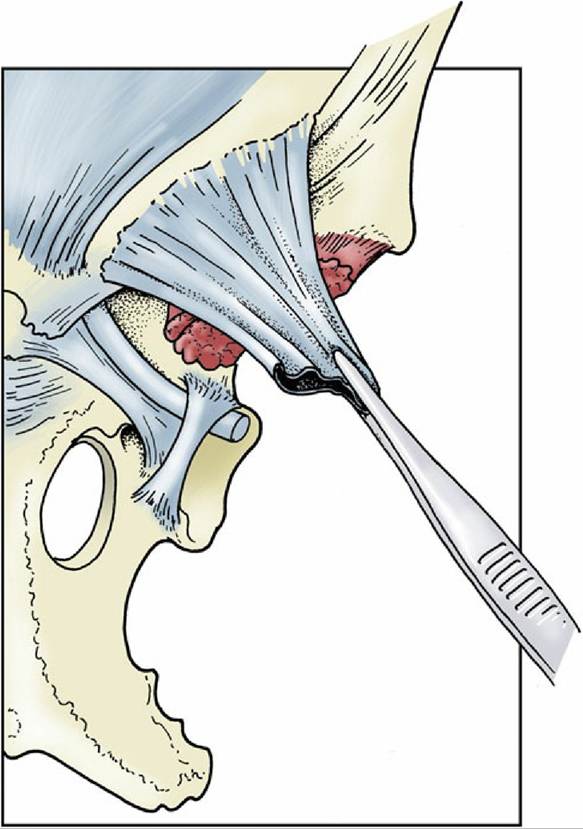
FIG. 21.5 The origin of the external spermatic fascia and femoral lamina from the margin of the superficial inguinal ring. (See Fig. 21.3 for orientation.)
The peritoneal sheath (vaginal tunic) of the spermatic cord contains a cavity that places the space about the testis in free communication with the peritoneal cavity of the abdomen. The communication occurs through the vaginal ring (≈3 cm long) situated midway in the deep inguinal ring (see Fig. 22.19A/10 and Fig. 22.24A and B) and identifiable per rectum in the stallion because of the constituents of the spermatic cord converging on it. The vaginal cavity provides a possible route for the herniation of intestines that may even reach the scrotum. This occurrence (indirect inguinal hernia) is a comparatively common sequel to castration.
Direct inguinal hernia, in which a loop of intestine forces an entry into the canal beside the vaginal tunic, is rare in horses.Incomplete descent of one or both testes (cryptorchidism) is common in the horse (p. 567). The testis may be retained within the abdomen or may enter but fail to leave the canal. Surgical correction may be indicated. It is therefore necessary to be aware that while the spermatic cord occupies a central position within the canal, the external pudendal artery, which must be treated with respect, occupies the caudomedial corner. The artery is accompanied by the genitofemoral nerve and a small vein. The larger (accessory) external pudendal vein makes a separate passage between the pectineus and gracilis muscles.
Innervation and Vascularization
The segmental innervation of the abdominal wall corresponds to the common pattern, and the minor variations are of little importance because paravertebral anesthesia is rarely practiced in the horse. The vascularization also follows the common pattern primarily. Mention may be made of a cranial branch of the deep circumflex iliac artery, which extends forward from the region of the coxal tuber between the muscles of the flank and is susceptible to injury during surgery in this region. The artery of the right side is also at risk in trocarization, which may be occasionally performed to relieve tympany of the cecal base. The abdominal floor and lower flank are served in the usual way by the cranial and caudal epigastric arteries and their superficial branches. No warning of the exact position of the vessels is available, and should vascular damage occur, control of the resulting hemorrhage may be troublesome and time consuming. It is said that the caudal epigastric artery is the vessel most often traumatized. The superficial thoracic or spur vein runs toward the axilla in the superficial fascia at the ventral edge of the cutaneous muscle. Connections with tributaries of the external pudendal vein make it available as an alternative drainage route from the prepuce or udder.