The Ventrolateral Abdominal Wall
Structure
The skin is thick over the flank but thins ventrally, particularly in heavy draft animals. It is especially thin in the cleft between the abdomen and thigh, where it is sparsely haired and glistens with the secretion of the sebaceous glands concentrated here.
In contrast, sweat glands are most abundant over the flank.A large subcutaneous bursa, a postnatal development, is present over the coxal tuber. Elsewhere the skin is closely adherent to the cutaneous trunci, which cover most of the flank, though not the abdominal floor. The upper border of the cutaneous muscle follows a line drawn from the withers to the stifle. The muscle is thickest cranially where it extends into the fascia over both the lateral and the medial aspects of the shoulder and arm. Caudally, it continues within the flank fold to end on the lateral femoral fascia. The cutaneous muscle is employed to twitch the skin to dislodge flies and other irritants. No detached bundles are associated with the prepuce, as in many species.
The loose fascia deep to the muscle conveys the cutaneous nerves and superficial vessels and encloses the subiliac lymph nodes. The deeper fascia consists largely of elastic tissue and, being yellowish, is also known as the tunica flava. It is well adapted to the passive support of the viscera and is thickest ventrally, where the burden is greatest. The dorsal part is easily dissected from the underlying muscle, but its ventral part exchanges fibers with the aponeurosis of the external oblique and is more tightly adherent. Bands detached from the deep fascia help support the prepuce or the udder. Careful suturing of this layer is necessary after abdominal surgery because its elastic nature tends to evert and draw apart the edges of a wound in the underlying muscle.
The linea alba, the prepubic tendon, and the associated structures have a particular importance in the horse.
The linea alba, mainly formed from the aponeuroses of the flank muscles, is considerably strengthened by longitudinal fibers. It is unequally developed along its length, being widest where it carries the umbilical scar (Fig. 21.2/d). It finally combines with the insertion tendons of the right and left rectus abdominis muscles to form a broad plate.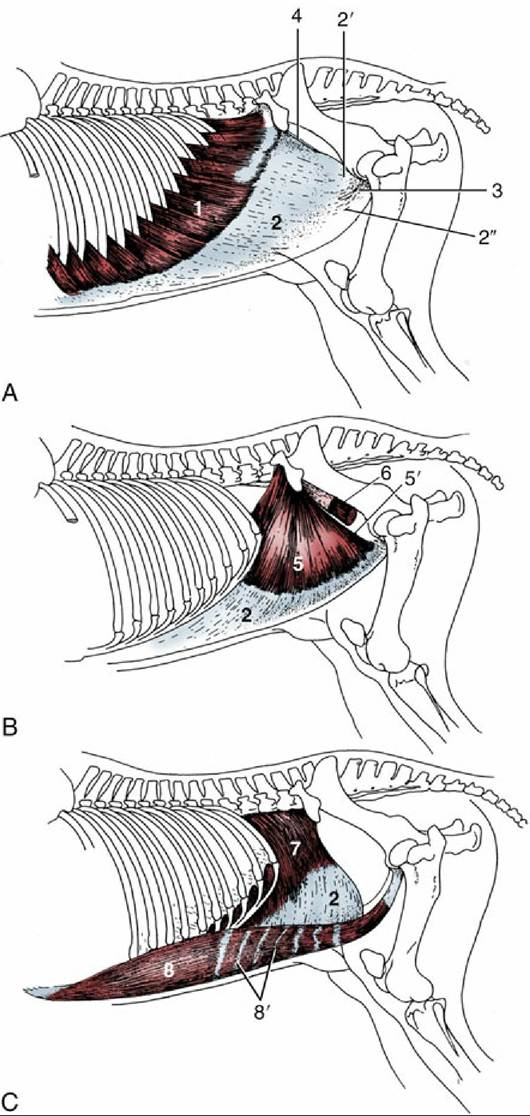
FIG. 21.1 The abdominal muscles and their skeletal attachments. 1, External abdominal oblique, muscular part; 2, aponeurotic parts of 1, 5, and 7; 2' and 2", pelvic and abdominal tendons of aponeurotic part, respectively; 3, superficial inguinal ring; 4, attachment of pelvic tendon of external oblique aponeurosis on iliopsoas and sartorius (“inguinal ligament”); 5, internal abdominal oblique, muscular part; 5', free caudal border forming the cranial margin of the deep inguinal ring; 6, iliopsoas, partly enclosed by iliac fascia; 7, transversus abdominis, muscular part; 8, rectus abdominis; 8', tendinous inscriptions.
The prepubic tendon* attaches abdominal muscles to the pelvic skeleton (Fig. 21.3/5). Once formed, the tendon ascends almost vertically toward the pelvic brim, but before reaching this, it is augmented by a strong transverse thickening. This thickening is mainly formed by the tendons of origin of the pectineus muscles (of the thighs), which arise from both the ipsilateral and contralateral pubic bones (from and medial to the iliopubic eminences) and which thus partly decussate across the midline. The caudal margins of the oblique abdominal muscles and the cranial part of the gracilis also contribute to the prepubic tendon. An important feature, peculiar to the horse, is the detachment from the caudolateral aspects of the prepubic tendon of the stout rounded cords that furnish accessory ligaments to the hip joints (Fig. 21.3/5' and Fig. 21.2). Each accessory ligament crosses the ventral surface of the pubis, enters the acetabulum through the notch in the rim, and inserts on the head of the femur beside the intracapsular ligament (of the head of the femur).
Each accessory ligament is predominantly composed of fibers from the two rectus muscles, and many fibers have decussated from the contralateral side. The ligaments appear to be the principal insertions of these muscles, which partly explains the restrictions on the movements permitted at the equine hips. It is postulated that the accessory ligaments are tensed by the weight of the abdominal contents and that this tension helps secure the femoral heads in place.Because the main weight of the abdominal organs is carried by the prepubic tendon, it follows that its rupture has the most dire consequences. This mishap, fortunately rare, is for obvious reasons most common in heavily pregnant mares.
The external abdominal oblique (Fig. 21.1/1) is the most extensive muscle of the flank. It arises from the thoracolumbar fascia and also from the lateral aspect of the thoracic wall (from the fifth rib caudally) by a series of digitations that engage with those of the serratus ventralis. The majority of its fascicles run caudoventrally to a broad aponeurosis that succeeds the fleshy part of the muscle along a line that sweeps from the coxal tuber toward the ventral end of the fifth rib.
Before insertion, the aponeurosis splits into (1) a large abdominal tendon that continues over the rectus to reach and insert on the linea alba and (2) a small pelvic tendon that inserts on the coxal tuber, the fascia over the iliopsoas and sartorius muscles, and the prepubic tendon (see Fig. 21.3). The split between the two tendons constitutes the superficial ring of the inguinal canal (Fig. 21.1/3). (The margins of the tendons are known as crura where they bound the opening, but the term is often misapplied to the tendons themselves.) The unnecessary term inguinal ligament, sometimes applied to the thickened caudodorsal edge of the pelvic tendon, confuses many descriptions of these structures. In fact, the prominence of this edge (Fig. 21.1/4) owes less to thickening than to tension through its connection with the fascia covering the iliopsoas and sartorius.
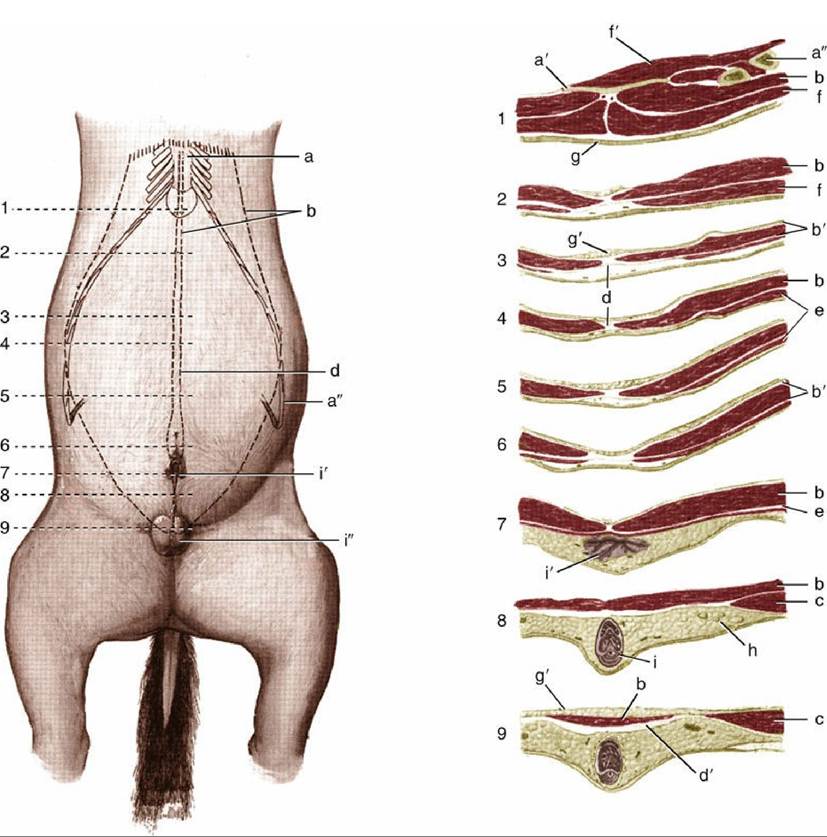
FIG. 21.2 Changes in the structure of the abdominal floor shown by means of a series of transverse sections (1-9) of a gelding. a, Sternum; a', xiphoid cartilage; a", costal arch; b, rectus abdominis; b', rectus sheath; c, internal oblique; d, linea alba; d', prepubic tendon; e, cutaneous trunci; f, pectoralis ascendens; f ', diaphragm; g, skin; g', fat; h, superficial inguinal lymph nodes; i, penis; i', prepuce; i", scrotum.
The internal oblique muscle (Fig. 21.1/5) radiates from an origin concentrated on the coxal tuber but extending onto the dorsocaudal edge of the pelvic tendon of the external oblique. Most bundles run cranioventrally to insert on the last costal cartilages or, via an aponeurosis that fuses with that of the external oblique, into the linea alba. Some pass ventrally and caudoventrally, and these cover the superficial inguinal ring on its internal aspect (Fig. 21.4/4). A caudal slip provides the cremaster, which passes onto the spermatic cord. The junction of the fleshy and aponeurotic parts of this muscle occurs more than halfway down the abdominal wall.
The transversus abdominis (Fig. 21.1/7) takes origin from the lumbar vertebrae and the medial aspect of the last ribs, ventral to the origin of the diaphragm. The fleshy part is continued by an aponeurosis that passes deep to the rectus abdominis to reach the linea alba. The transversus, the least extensive of the three muscles of the flank, does not extend caudal to the level of the coxal tuber; the internal lamina of the rectus sheath is thus deficient caudally.
The rectus abdominis (Fig. 21.1/8) arises from the fourth to ninth costal cartilages and the adjacent part of the sternum. It inserts by way of the prepubic tendon and accessory ligaments. The muscle, relatively narrow over the thorax, widens considerably over the abdomen before again narrowing toward its insertion (see Fig.
21.2/b).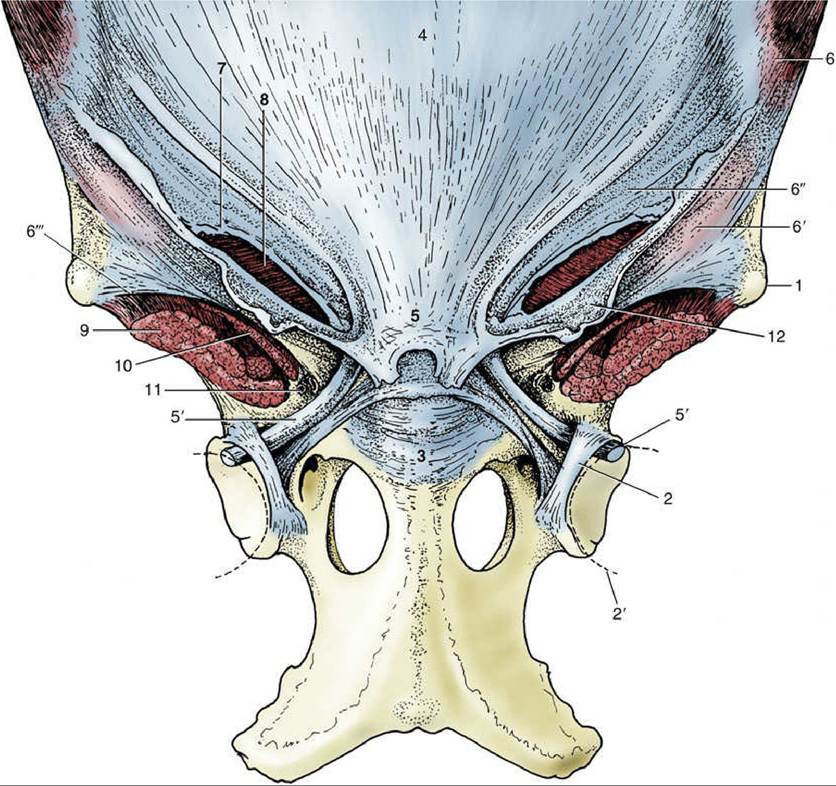
FIG. 21.3 The attachment of the abdominal muscles on the pelvis and the prepubic tendon. 1, Coxal tuber; 2, transverse acetabular ligament; 2', femoral head; 3, pubis; 4, tunica flava over linea alba; 5, prepubic tendon; 5', accessory ligament; 6, external abdominal oblique; 6' and 6", pelvic and abdominal tendons of external oblique aponeurosis, respectively; 6'", attachment of pelvic tendon of external oblique aponeurosis on sartorius and iliopsoas (“inguinal ligament”); 7, superficial inguinal ring; 8, internal abdominal oblique; 9, iliopsoas; 10, sartorius; 11, vascular lacuna containing femoral vessels; 12, femoral fascia (lamina).
Although the functions of the abdominal muscles are the same in all species, the expiratory role is relatively more important in the horse because the elasticity of the lungs is frequently reduced in older horses. Contraction of the abdominal musculature is then more necessary to return the viscera, and thus the diaphragm, from the inspiratory position. In this action the junction between the fleshy and aponeurotic parts of the external oblique muscle becomes visible as the so-called heave line.
The fascia that supports the peritoneum is often heavily but unequally infiltrated with fat. This layer, which may be 6 cm or more thick in horses in good condition, must be taken into account when making and closing a surgical incision.