The Initiation of Exercise Involves an Interplay of Local and Neural Changes That Increases Cardiac Output and Delivers Increased Flow to Exercising Muscle
As discussed in Chapter 24, local metabolic control mechanisms dilate skeletal muscle arterioles during exercise. Metabolic products accumulate in exercising muscle, and the local oxygen concentration decreases.
The metabolic products and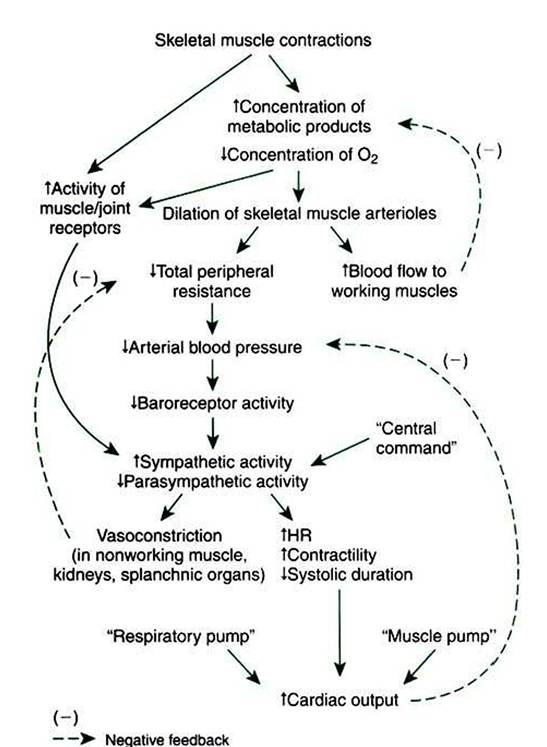
FIGURE 26-8 Cardiovascular responses to exercise involve a complex interplay of local metabolic control mechanisms: central command, reflexes, and the blood-pumping effects of muscle contraction and respiration.The overall result is increased blood flow in exercising muscle, decreased blood flow in the noncritical organs, decreased total peripheral resistance, increased cardiac output, and (normally) maintenance of arterial blood pressure near its normal level. HR, Heart rate.
hypoxia both cause dilation of the arterioles within the exercising muscle. This vasodilation is a local response, not dependent on nerves or hormones. The result is an increased blood flow to the exercising muscle (active hyperemia). The increased blood flow delivers more oxygen and removes some of the accumulated metabolic vasodilating products. In this way, muscle blood flow is matched to metabolic rate (Figure 26-8, top).
Metabolic control of blood flow in exercising muscle can succeed only if arterial blood pressure is maintained at a level sufficient to provide the needed additional blood flow. This necessitates a substantial increase in cardiac output and, in extreme exercise, vasoconstriction in the noncritical organs (which makes more blood flow available for the exercising muscle and other critical organs). These adjustments are brought about by three neural mechanisms: central command, the exercise reflex, and the arterial baroreflex.
Central command is a psychogenic effect. In preparation for exercise (and continuing during exercise) the CNS increases sympathetic activity to the heart and blood vessels and decreases parasympathetic activity to the heart.
The sympathetic and parasympathetic changes are graded, depending on the intensity of the exercise. In effect, central command represents a “guess” by the brain as to the levels Ofsympathetic and parasympathetic activity that will be needed during the exercise to match cardiac output to the needs of the systemic organs.The exercise reflex is the second mechanism that helps set the level of sympathetic and parasympathetic activity during exercise. The exercise reflex is initiated by specialized nerve endings within muscles and joints. An increase in muscular work and in the movement of the body joints activates these muscle and joint receptors. The resulting increased afferent neural activity initiates a reflex increase in sympathetic (and decrease in parasympathetic) efferent drive. Although the mechanism for excitation of the muscle and joint receptors is not completely understood, it is clear that the activation of these receptors is necessary to keep blood pressure from falling during exercise.
The arterial baroreceptor reflex is the third major controller of sympathetic and parasympathetic activity during exercise. The baroreflex serves to fine-tune autonomic drive to the heart and arterioles to keep arterial pressure at its set point. If central command and the exercise reflex do not set sympathetic activity to a sufficiently high level during a particular bout of exercise, arterial pressure falls below normal. The arterial baroreceptors detect this low pressure, and the baroreflex responds by increasing sympathetic activity. Conversely, if central command and the exercise reflex set sympathetic activity too high, arterial pressure rises above normal. The response of the baroreflex is to decrease sympathetic activity.
In effect, central command and the exercise reflex initiate the autonomic adjustments for exercise, and the arterial baroreflex performs the fine-tuning to keep arterial pressure near its set point (Figure 26-8).
Two additional, nonneural mechanisms also help to increase the cardiac output during exercise.
The first of these is the muscle pump (Figure 26-9). When skeletal muscles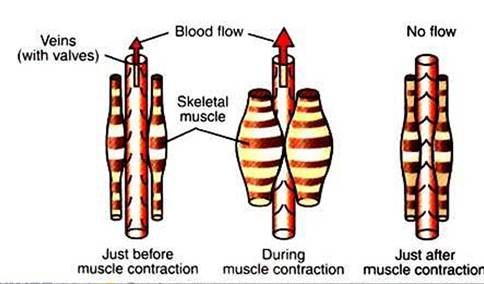
FIGURE 26-9 During dynamic exercise, the rhythmical contractions of the skeletal muscles squeeze venous blood back toward the central circulation.This so-called muscle pump helps increase central venous pressure in an exercising animal.
contract, they tend to squeeze down on the blood vessels contained within them. One consequence of this is the tendency for a muscle to restrict its blood flow during a sustained contraction (see Chapter 24). If the contractions are rhythmical, however, each contraction causes blood to be expelled out of the muscle veins and thus toward the central circulation. Minimal backflow of blood occurs from the central circulation into the veins during muscular relaxation because the veins have one-way valves within them. Thus, by massaging the veins, exercising muscles exert a pumping action that displaces venous blood toward the central circulation and increases central venous pressure. The consequence is an increase in ventricular preload above the level that would otherwise exist.
The second nonneural mechanism that helps to increase cardiac output during exercise is the respiratory pump. Vigorous exercise involves an increase in the rate and the depth of respiration. During each inspiration, a Subatmospheric pressure is generated within the intrapleural space. This negative pressure distends the airways of the lungs and expands them. It also increases the distending pressure on the central veins and the heart. Distention of the central veins and heart helps promote the flow of blood from the abdominal veins into the central veins and heart. In addition, the diaphragm muscle moves caudally during inspiration and compresses the abdominal organs. The resulting increase in intraabdominal pressure “squeezes” blood out of the abdominal veins and back toward the central veins.
Overall, the respiratory pumping action helps to increase venous return, central venous volume, and ventricular preload during exercise.Cardiac output can increase four to six times its resting level during vigorous exercise as a result of the combined effects of sympathetic and parasympathetic responses, the muscle pump, and the respiratory pump. Note that the success of the mechanisms that increase cardiac output during exercise depends on the heart's ability to respond normally both to increased sympathetic drive and to increases in preload. As mentioned earlier, during heart failure the autonomic mechanisms available to increase cardiac contractility and heart rate are invoked simply to maintain a normal cardiac output at rest. Therefore the autonomic nervous system in a patient with heart failure has a limited ability to bring about further increases in cardiac output during the initiation of exercise. For this reason, patients with heart failure typically exhibit exercise intolerance.
Maximal exercise ability in normal humans and animals appears to be limited by cardiac output. That is, the respiratory system can oxygenate as much blood as the heart can deliver to the lungs, and skeletal muscle can take up and metabolize as much oxygen as the heart can deliver to it. When cardiac output has reached a maximal level, however, oxygen transport from the lungs to the skeletal muscle also is maximized. This sets the upper limit to the level of exercise that can be sustained.