The Blood VoIume Lost in Hemorrhage Is Restored Through a Combination of Capillary Fluid Shifts and Hormonal and Behavioral Responses
Hemorrhage causes both venous and arterial pressures to fall below normal, so capillary hydrostatic pressure also falls below normal throughout the body. This alters the balance of hydrostatic and oncotic pressures acting on water in a direction that favors reabsorption of interstitial fluid back into the capillaries (Figure 26-6).
The volume of interstitial fluid that can be reabsorbed by this process in 1 hour is approximately 10% of the volume lost in the hemorrhage. However, the rate of reabsorption of interstitial fluid becomes limited after 3 to 4 hours. As interstitial fluid is reabsorbed, there is a decrease in interstitial fluid hydrostatic pressure (it becomes even more negative than normal), and this opposes further reabsorption. Also, as interstitial fluid is reabsorbed, the interstitial fluid protein concentration increases because proteins in the interstitial fluid are not reabsorbed. The resulting increase in interstitial fluid oncotic pressure also opposes further reabsorption. Despite these limits, the reabsorption of interstitial fluid is an important compensation for hemorrhage in the first few hours.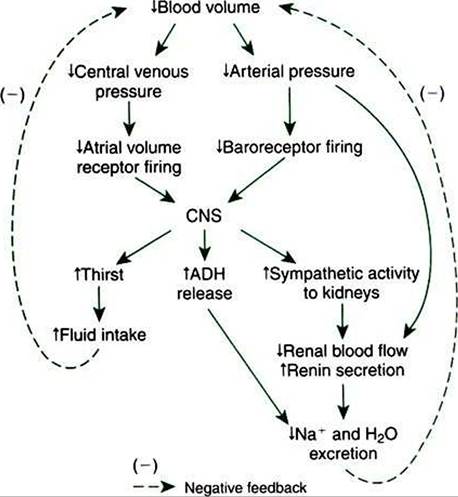
FIGURE 26-7 Behavioral and humoral responses after hemorrhage include increased fluid intake and retention of body fluid and electrolytes. ADHf Antidiuretic hormone; CNSf central nervous system.
A complication arising from the reabsorption of interstitial fluid after hemorrhage is that the reabsorbed fluid contains no plasma proteins or blood cells. Therefore the proteins and cells already in the bloodstream are diluted as interstitial fluid is reabsorbed. The concentration of plasma proteins in blood decreases, as does the hematocrit. This is why a decreasing hematocrit over a few hours in an otherwise-normal patient is presumptive evidence that a hemorrhage has occurred recently or is continuing to occur.
In the absence of an obvious hemorrhage, such a patient should be examined for evidence of internal bleeding.The restoration of blood volume after hemorrhage also involves hormonal and behavioral responses (Figure 26-7). As mentioned, hemorrhage leads to a decrease in the action potential frequency of both the arterial baroreceptors and the atrial volume receptors. The immediate, compensatory reflex responses have already been described (see Figure 26-5). The arterial baroreflex and the atrial volume receptor reflex also trigger important hormonal and behavioral effects. The increase in sympathetic activity (coupled with a decrease in arterial pressure) acts on the kidneys to increase their release of the hormone renin. As mentioned in Chapter 25, renin works through the additional hormones angiotensin and aldosterone to decrease sodium excretion by the kidneys. Decreased activity of the baroreceptors and atrial volume receptors also triggers increased ADH secretion from the pituitary gland. ADH circulates to the kidneys, where it reduces urine formation. Through the combined actions of renal vasoconstriction, the renin-angiotensin-aldosterone system, and ADH, sodium excretion and water excretion are both decreased. Note that these actions conserve the available blood volume after hemorrhage, but they do not restore it to normal. The actual restoration of blood volume after hemorrhage requires increased fluid intake. The baroreceptor reflex and the atrial volume receptor reflex act through the hypothalamus to increase the sensation of thirst. If water is available, fluid intake increases until the lost blood volume is restored to normal. This may take 1 to 2 days.
The final compensations for hemorrhage involve the restoration of the lost plasma proteins and blood cells. The plasma proteins are synthesized by the liver, and the blood cells are produced by the bone marrow. The time required may be several days for the plasma proteins and a few weeks for the blood cells.
The preceding discussion focused on the effects of severe hemorrhage. All the same compensations occur to a lesser degree after mild hemorrhage. For example, when a human donates blood, about 10% of the blood volume (0.5 L) is removed. A∏ the compensations just described are evident after this 10% hemorrhage.
In humans and in some large animals, the transition from a supine to a standing posture elicits many of the same cardiovascular responses as hemorrhage. You can understand the reason for this if you consider the effect of gravity on the blood contained within the blood vessels of the body. In a standing subject, gravity increases the distending pressure in the dependent vessels (those below heart level), particularly in the leg vessels. The gravitational effect does not cause much accumulation of blood in the arteries and arterioles because these vessels are not easily distensible (i.e., they have low compliance). However, the gravitational effect causes a significant distention of the dependent veins because of their much greater compliance. The extra blood in the dependent veins is blood that would otherwise have returned to the central circulation. Therefore, in an upright subject, there is a decrease in central blood volume and central venous pressure, just as there would be after hemorrhage. Furthermore, upright posture causes decreased cardiac filling, decreased stroke volume, decreased cardiac output, and so on. In a normal human the assumption of an upright posture is equivalent to a 10% hemorrhage. In small animals the gravitational effect of standing is negligible. In large animals, such as horses and cattle, the volume of blood that pools in the leg veins is minimized by the relatively small size of veins in the extremities.