» The Larynx
The larynx is suspended by the hyoid apparatus and is partly contained within the intermandibular space (see Fig. 4.8). Although few distinguishing features of the cartilages are important, attention must be drawn to the deep notch in the ventral part of the thyroid cartilage because this provides very convenient access to the interior after incision of the cricothyroid ligament.
A prominence rostral to the notch and the ventral part of the cricoid arch provide the necessary landmarks (see Fig. 4.13/7), but the basihyoid may also be used to confirm the site of the initial skin incision. The normally retrovelar position of the leaf-shaped epiglottis has been pointed out (Fig. 18.11/H).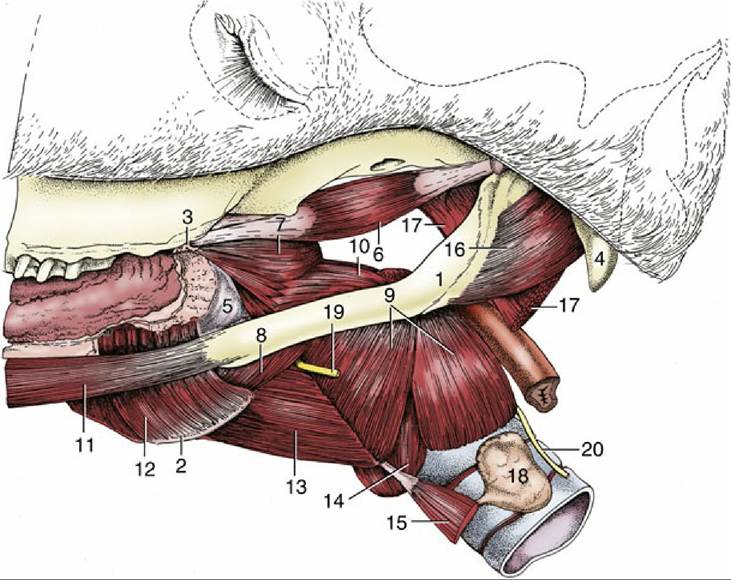
FIG. 18.30 Muscles of the pharynx, soft palate, and hyoid apparatus. 1, Stylohyoid; 2, thyrohyoid; 3, hamulus of pterygoid bone; 4, paracondylar process; 5, buccopharyngeal fascia; 6, tensor veli palatini; 7, rostral pharyngeal constrictor; 8, middle pharyngeal constrictor; 9, caudal pharyngeal constrictor (thyropharyngeus and cricopharyngeus); 10, stylopharyngeus caudalis; 11, styloglossus; 12, hyoglossus;
13, thyrohyoideus; 14, cricothyroideus; 15, sternothyroideus; 16, occipitohyoideus; 17, longus capitis (stump); 18, thyroid gland; 19, cranial laryngeal nerve; 20, caudal (recurrent) laryngeal nerve.
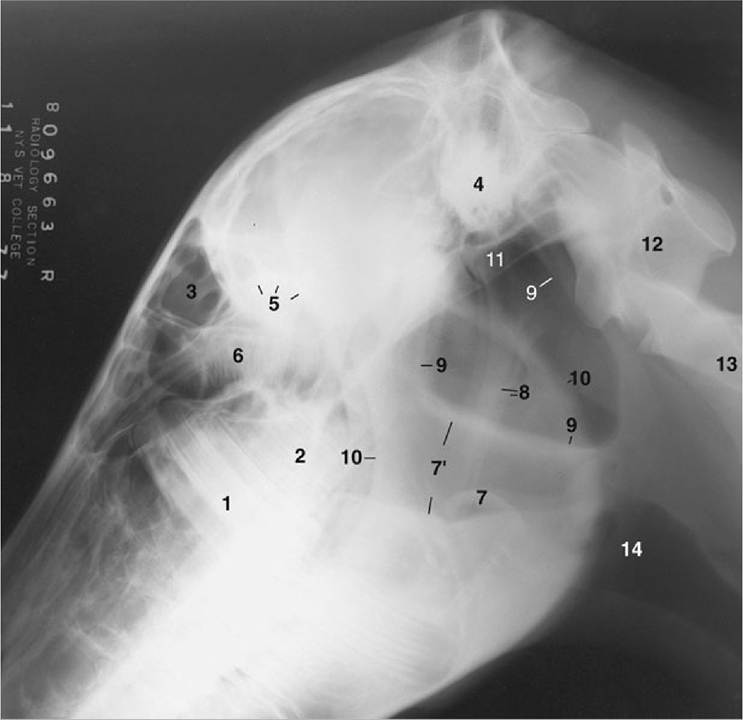
FIG. 18.31 Lateral radiographic view of the head to show the position of the guttural pouches (9) in a horse 1½ years old (estimated). 1, M1; 2, unerupted M2; 3, frontal sinus; 4, petrous temporal bone; 5, caudal border of orbit; 6, ethmoid labyrinth; 7, epiglottis; 7', nasopharynx; 8, stylohyoid bones; 9, borders of guttural pouches; 10, rostral and caudal borders of mandible; 11, base of skull; 12, atlas; 13, axis; 14, larynx.
The mucosa forms outpouchings (ventricles) that pass laterally between the vocal and vestibular folds but remain within the protection of the thyroid laminae. The ventricular entrance is sufficiently large to admit the bur that is used to evert the sac in one of the "roaring" operations (Fig. 18.35/1).
FIG. 18.32

Position of the guttural pouch in relation to the skull and stylohyoid. 1, Lateral compartment of
guttural pouch; 2, medial compartment of guttural pouch; 3, stylohyoid.
The interference with the normal dilation of the glottis during inspiration diminishes the respiratory efficiency. The condition known as roaring, from the strident sound emitted at inspiration, is commonly seen in high-performance horses. In its severe form it is characterized by unilateral adduction of the arytenoid cartilage and vocal cord; in less severe forms it is identified by limited abduction of these structures. The abnormal sound is produced by passive vibration of a lax vocal cord in the airstream as a result of dysfunction or even atrophy of part of the intrinsic laryngeal musculature. The pathology is almost always on the left side and is initially seen in the cricoarytenoideus dorsalis, the abductor muscle of the cartilage, before involving other adductors in the larynx (see Fig. 4.15/5). The asymmetry in incidence may be due to differences in the course of the right and left recurrent laryngeal nerves. The change in the contour of the larynx resulting from loss of function of the cricoarythenoideus dorsalis can be appreciated with palpation. The hollowed space above the arytenoid cartilage makes the muscular process of the cartilage more prominent.
The roaring can be relieved through the reinforcement of the wasted dorsal cricoarytenoideus muscle by a suture tightened to fix the arytenoid cartilage in permanent abduction. An older alternative was the eversion and excision of the lateral laryngeal ventricle in the expectation that the resulting scar tissue would bind this cartilage to the thyroid cartilage.
Both operations result in tightening of the vocal fold and widening of the glottic cleft. Neither operation effects a cure of the condition, which has human and canine parallels. Other defects, such as partial collapse of an arytenoepiglottic fold or prolapse of the cricotracheal membrane, may also cause obstruction. It is noteworthy that multiple defects, possibly involving nasal, pharyngeal, and laryngeal levels, are quite common. Recently a syndrome of deformities that may afflict the derivates (the pharynx, larynx, and upper esophagus) of the fourth branchial arch has been described.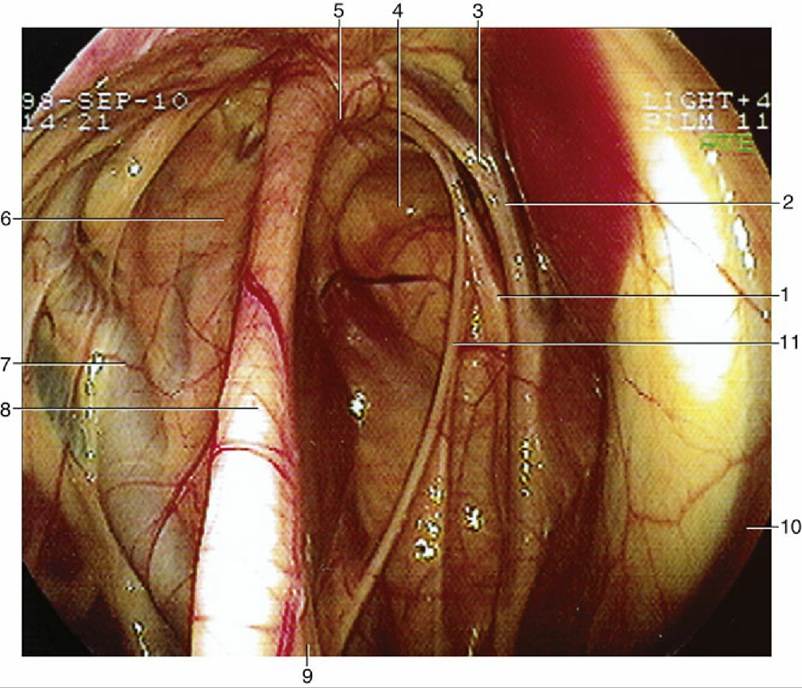
FIG. 18.33 Endoscopic view of the interior of the guttural pouch. 1, Hypoglossal nerve; 2, vagus nerve;
3, internal carotid artery; 4, medial compartment; 5, articulation of the stylohyoid and petrous temporal bone; 6, lateral compartment; 7, external carotid artery; 8, stylohyoid bone; 9, stylopharyngeus muscle; 10, longus capitis muscle; 11, glossopharyngeal nerve.

FIG. 18.34 Tympany of the guttural pouch (arrow).
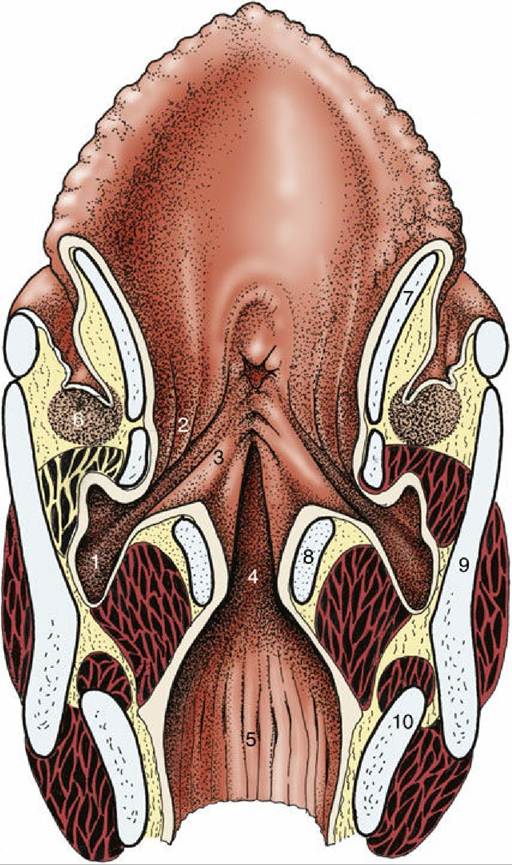
FIG. 18.35 Dorsal section of the larynx. 1, Laryngeal ventricle; 2, vestibular fold with ventricularis; 3, vocal fold with vocalis; 4, glottic cleft; 5, infraglottic cavity; 6, caudal end of palatine tonsil; 7, epiglottic cartilage; 8, arytenoid cartilage; 9, thyroid cartilage; 10, cricoid cartilage.