The Guttural Pouch
The guttural pouch, a diverticulum of the auditory tube, is found in the horse and other Perissodactyla* (Fig. 18.31/9). It is formed by the escape of the mucosal lining of the tube through a ventral slit between medial and lateral supporting cartilages and attains a capacity of some 300 to 500 mL.
It lies between the base of the skull and atlas dorsally and the pharynx and commencement of the esophagus ventrally; it is covered laterally by the pterygoid muscles and parotid and mandibular glands. Medially, the dorsal parts of the right and left sacs are separated by the ventral straight muscles of the head, but below this they meet, forming a thin median septum. The floor lies mainly on the pharynx but also covers and is molded to the stylohyoid, which raises a ridge that incompletely divides the medial and lateral compartments (Fig. 18.32).More detailed relations include several cranial nerves and arteries that lie directly against the pouch as they pass to and from foramina in the caudal part of the skull. The glossopharyngeal, vagus, accessory, and hypoglossal nerves; the continuation of the sympathetic trunk beyond the cranial cervical ganglion; and the internal carotid artery are closely related for a stretch and together raise a mucosal fold that indents the medial compartment from behind. This is a conspicuous feature when the interior of the pouch is viewed endoscopically (Fig. 18.33/4). The facial nerve has a more limited contact with the dorsal part of the pouch. The large external carotid artery passes ventral to the medial compartment before crossing the lateral and then rostral walls of the lateral compartment (Fig. 18.33/6) in its approach (as the maxillary artery) to the alar canal. The pouch also directly covers the temporohyoid joint.
Function of the Guttural Pouch: The data now identify the pouch as a mechanism for cooling the cerebral blood supply, a mechanism that is peculiar to the horse (at least among domestic species) and additional to other devices found in mammals generally.
The extensive contact between the extracranial part of the internal carotid artery and the exceedingly thin pouch wall cools the major (internal carotid) contribution to the cerebral blood supply. No local differences in blood temperature were registered in the resting animal, but a significant drop in temperature (of about 2°C) at the distal end of the artery was demonstrated in horses engaged in 15 minutes of strenuous exercise.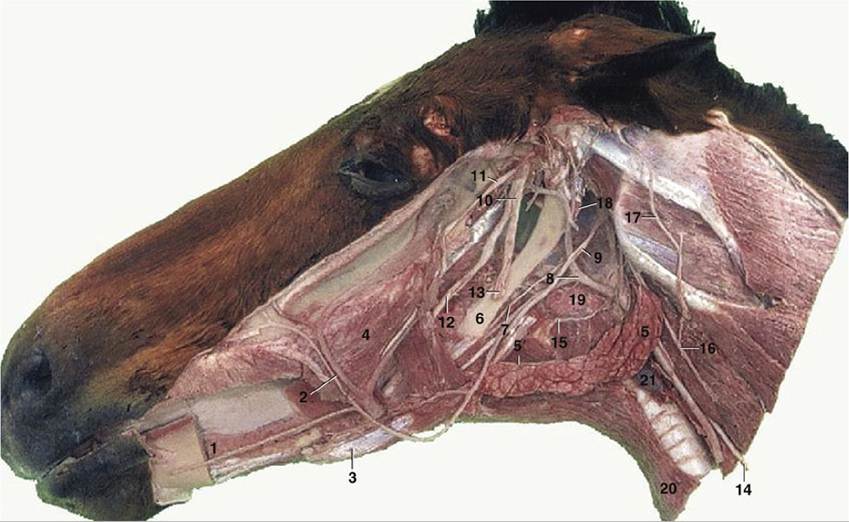
FIG. 18.26 Deep dissection of the head. The mandible and masticatory muscles have been removed. 1, Sublingual gland; 2, facial artery and vein; 3, rostral belly of digastricus; 4, buccinator; 5, mandibular gland; 5', mandibular duct; 6, stylohyoid; 7, glossopharyngeal nerve (n.); 8, linguofacial artery; 9, hypoglossal n.; 10, mandibular n.; 11, masseteric n.; 12, lingual n.; 13, inferior alveolar n., cut where it enters the mandibular foramen; 14, vagus and sympathetic trunk; 15, cranial laryngeal n.; 16, dorsal
branch of spinal accessory n.; 17, great auricular n.; 18, guttural pouch; 19, medial retropharyngeal lymph nodes; 20, sternohyoideus; 21, thyroid gland.
Clinical Conditions of Guttural Pouch
The mucous secretion of the lining normally drains into the pharynx through the pharyngotubal opening (Fig. 18.11/8) placed at the rostral end of the pouch, the most dependent part when the head is lowered. The connection opens when the horse swallows, and grazing normally promotes drainage. When the exit is blocked or the secretion accumulates for any reason, the pouch distends, producing a palpable, often visible swelling behind the jaw (Fig. 18.34). The guttural pouch may be infected with bacteria such as Streptococcus equi equi from the neighboring retropharyngeal lymph nodes. Mycotic infections of the guttural pouch also occur. The clinical signs include painful swelling of the parotid region, abnormal carriage of the head and neck, and nasal discharge.
More frequent possible sequelae include inflammation of the middle ear (by extension of infection along the auditory tube), epistaxis (nasal bleeding) from erosion of the internal carotid artery, difficulty in swallowing following involvement of the glossopharyngeal and vagus nerves (or their pharyngeal branches), and laryngeal hemiplegia ("roaring") following vagus involvement. Other signs such as nasal congestion, drooping of the upper eyelid, pupillary constriction, sweating, and increased skin temperature over the affected side of the head and neck that result from the involvement of the sympathetic nerve form Horner syndrome. The facial and hypoglossal nerves and the external carotid artery are usually spared.The pouch can be inspected or drained via the pharyngotubal opening or approached by open surgery through the Viborg triangle, which is an area bounded by the caudal border of the mandible (more deeply, the occipitomandibularis), the tendon of the sternocephalicus, and the linguofacial vein. The distance between the triangle and the pouch is greatly reduced when the pouch is enlarged. An alternative, more dorsal approach, involving reflection of the parotid gland is also employed.
Hemorrhage from the internal carotid artery is frequently fatal unless treated promptly by closure of the vessel on each side of the leak. A proximal ligature is easily applied, but direct access to a site distal to the lesion may be impossible. Recourse may then be had to a balloon-tipped catheter, which is introduced beyond the proximal ligature and advanced into the siphon-like formation that the artery displays immediately before entering the cranial cavity. The catheter is left in place until it is judged that thrombosis will have sealed the damaged segment of the artery.
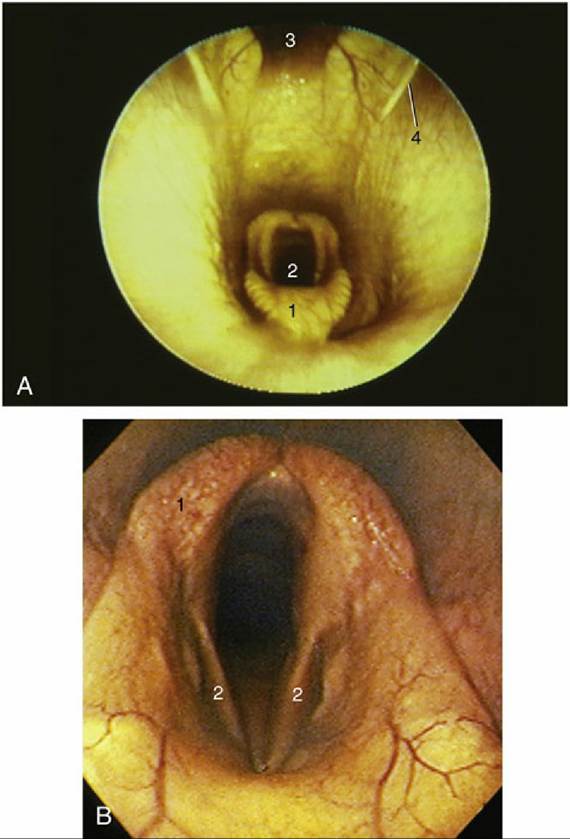
FIG. 18.27 (A) Endoscopic view of equine nasopharynx. 1, Epiglottis; 2, laryngeal entrance; 3, pharyngeal recess; 4, entrance to auditory tube.
(B) Endoscopic view of larynx. 1, Arytenoid cartilage; 2, left and right vocal folds.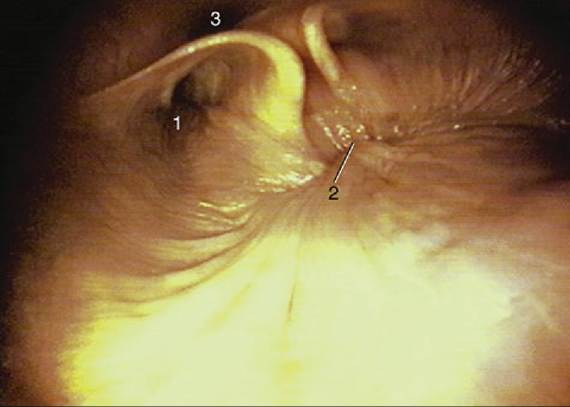
FIG. 18.28 Endoscopic view of the caudal part of equine nasopharynx (foal). 1, Entrance to auditory tube; 2, closure of the intrapharyngeal ostium between the nasopharynges and laryngopharynges (during swallowing); 3, cartilage flange supporting the auditory tube.
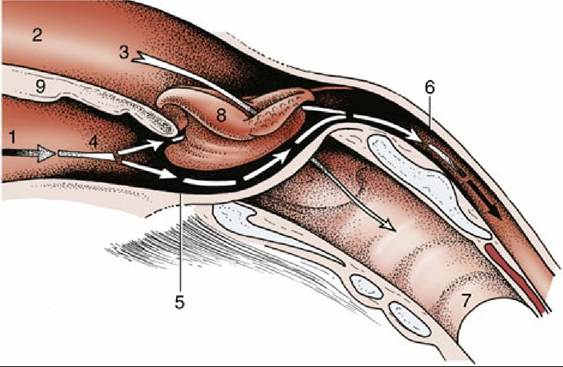
FIG. 18.29 The communications of the pharynx, rostrally with the oral and nasal cavities and caudally with the esophagus (schematic). The broken arrows mark the digestive pathway; the unbroken arrow marks the respiratory pathway. 1, Oral cavity; 2, nasal cavity; 3, nasopharynx; 4, oropharynx; 5, laryngopharynx; 6, esophagus; 7, trachea; 8, epiglottis, laryngeal entrance; 9, soft palate.
In foals, malfunction of the pharyngotubal opening may result in the pouch becoming distended with air to the extent that a swelling is visible externally (Fig. 18.34). It appears that in some horses there may be a redundancy of the mucosal fold (plica salpingopharyngea) that is normally present at the entry of the tube. In these individuals the excess mucosa creates a one-way valve that allows air to be drawn into the pouch but not expelled from it. Unilateral tympany may be relieved by forcing an opening in the median septum so that both pouches communicate with the pharynx through a single opening. When swelling is bilateral, an alternative surgical method has to be used.