» The Liver
The liver (see also pp. 125-128) is relatively large, weighing about 450 g on average, and accounts for 3% to 4% of the body weight. It is almost entirely intrathoracic, occupying a central position with only a slight bias to the right side (Figs.
14.10/2, 14.23, 14.25 and 14.26). The modest asymmetry is caused by the enlargement of the caudate process beneath the last ribs, where it makes contact with the right kidney (Fig. 14.13/9). The ventral border extends across the costal arches and would be palpable were it not for the fat within the falciform ligament and the taut rectus muscles. Even so, it may be appreciated when significantly enlarged. The liver in dogs and cats is deeply divided by fissures extending from the ventral margin; the pattern, the relative extents, and the names of the lobes may be obtained from Fig. 3.53.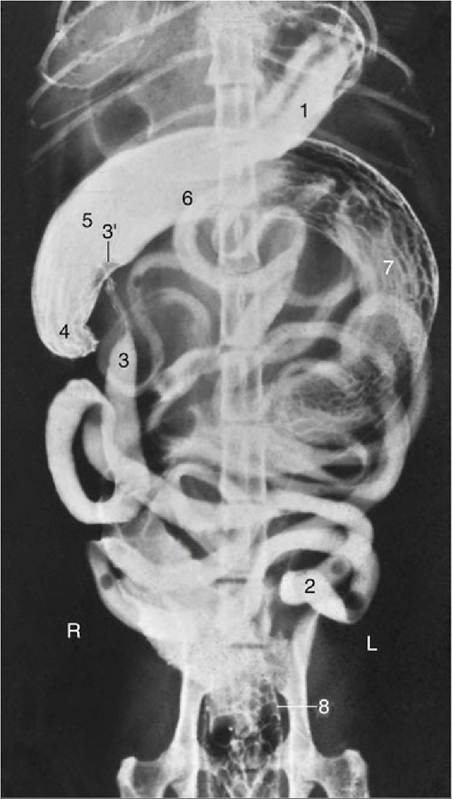
FIG. 14.20 Ventrodorsal radiographic view of the feline abdomen after administration of a barium suspension. 1, Residue of barium in stomach; 2, jejunum; 3, ileum; 3', ileal papilla; 4, cecum; 5-7, colon— the long descending part (7) has curved far to the right in this animal; 8, rectum; L, left; R, right.
The cranial surface conforms to the curvature of the diaphragm with which it is in extensive contact and to which it is secured by the caudal vena cava embedded in the dorsal border (Fig. 14.25 and 14.26). The attachment to the tendinous center of the diaphragm is completed by right and left coronary ligaments caudolateral to the vein. Most of the liver can therefore be retracted during surgery to expose the diaphragm. The gallbladder is sunk deeply between the lobes, just to the right of the median plane opposite the eighth intercostal space. It usually makes contact with the diaphragm and always appears at the visceral surface, although it is too short to reach the ventral border (Fig.
14.26/8).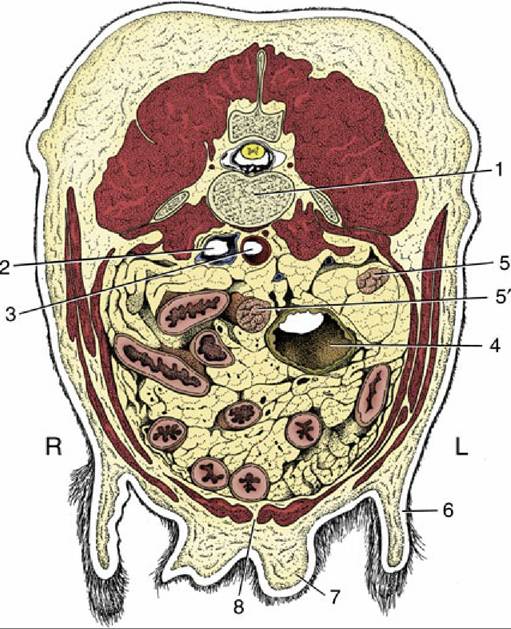
FIG. 14.21 Transverse section of the canine abdomen at the level of the fourth or fifth lumbar vertebra.
1, Lumbar vertebra; 2, caudal vena cava; 3, aorta; 4, descending colon; 5 and 5', right and left uterine horns; 6, flank fold; 7, mammary gland; 8, linea alba; L, left; R, right.
The visceral surface, though concave, is made irregular by various visceral impressions. The largest of the impressions is made by the body of the stomach to the left of the median plane, and the pyloric part and duodenum produce a narrower impression leading away to the right (Fig. 14.13/7). The other prominent impression, involving the right lateral lobe and caudate process, is made by the right kidney. Other organs that may touch the liver, especially when the stomach is empty, leave no mark, except the pancreas, which attaches near the porta.
The attachments on the visceral surface are larger but looser and are part (as mentioned earlier) of the lesser omentum. The hepatogastric ligament contains the bile duct as well as the hepatic artery, the portal vein, lymphatic vessels, and nerves. Once the hepatic ducts receive the cystic duct from the gallbladder, the duct is known as the common bile duct (ductus choledochus). In dogs, it runs from the hilus to the duodenum. Its terminal portion continues for some 2 cm within the duodenal wall before opening by the side of the pancreatic duct on the major duodenal papilla, a small elevation 2 to 3 mm high, caudally directed, and located about 3 to 6 cm from the pylorus in both dogs and cats.
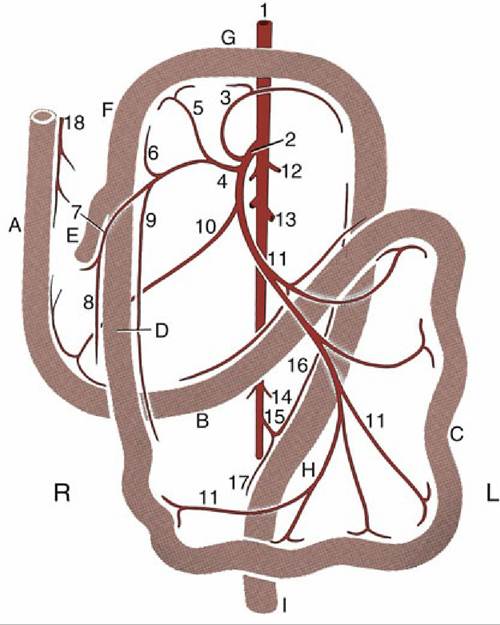
FIG. 14.22 The blood supply of the intestinal tract, ventral view; schematic. A, Descending duodenum; B, ascending duodenum; C, jejunum; D, ileum; E, cecum; F, ascending colon; G, transverse colon; H, descending colon; I, rectum; 1, abdominal aorta; 2, cranial mesenteric artery (a.); 3, middle colic a.; 4, ileocolic a.; 5, right colic a.; 6, colic branch of ileocolic a.; 7, cecal a.; 8, antimesenteric ileal branch; 9, mesenteric ileal branch; 10, caudal pancreaticoduodenal a.; 11, jejunal arteries (aa.); 12,
Phrenicoabdominal aa.; 13, renal aa.; 14, testicular (ovarian) aa.; 15, caudal mesenteric a.; 16, left colic a.; 17, cranial rectal a.; 18, cranial pancreaticoduodenal a.
Biopsy samples of liver tissue may be obtained by puncture caudal to the xiphoid process; the instrument is directed toward the large left lobe to avoid the gallbladder (Fig. 14.5).
In survey radiographs of the abdomen the liver appears as a large, uniformly dense shadow from which its size, relative to the species norm, may be crudely assessed. When such an assessment is made, it is necessary to be mindful that the liver is more or less completely "intrathoracic" in large, deep-chested breeds, whereas a more appreciable portion projects beyond the costal arch in dogs of less extreme conformation. In overindulged cats the liver may be displaced dorsally and away from the abdominal floor owing to the deposition of excessive fat within the falciform ligament.
The liver is a soft organ with very little fibrous tissue. This characteristic makes ligation of the blood vessels very difficult in hepatic surgery.
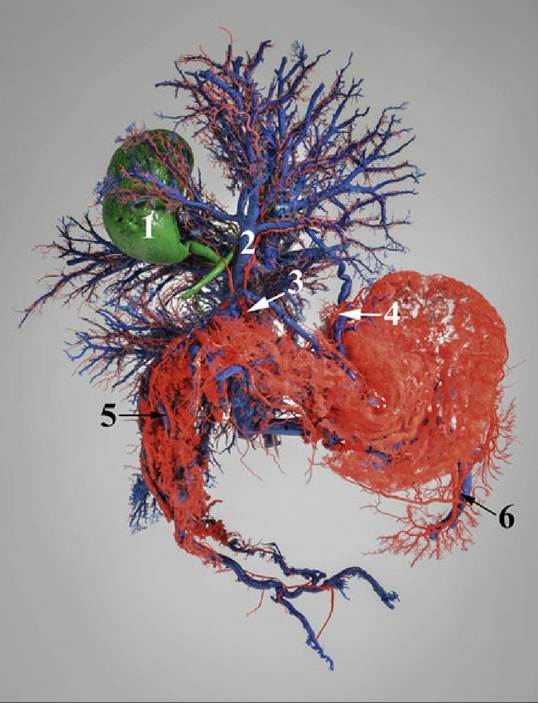
FIG. 14.23 Corrosion cast of the celiac artery and the caudal vena cava of the dog. 1, Gallbladder; 2, Hepatic vein; 3, Hepatic artery; 4, Left gastric artery and vein; 5, Cranial pancreaticoduodenal artery and vein; 6, Splenic artery and vein.
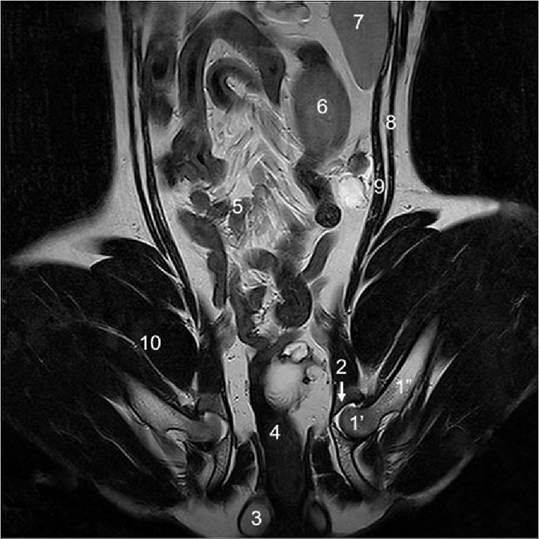
FIG. 14.24 A frontal section of a dog at the level of femur head; Magnetic Resonance Imaging (MRI).
Notice the femur head (1') and shaft (1”), acetabulum (2), anal sacs (3), rectum (4), jejunal loops (5), left kidney (6), spleen (7), external oblique (8) and internal oblique (9) abdominal muscles, and quadriceps muscles (10) of the thigh.