THE LYMPHATIC STRUCTURES WITHIN THE THORAX
The lymphatic drainage of the thorax is complicated and variable. Not every node is present in every animal, and some may be placed so that it is difficult to assign them to a particular group.
A series of small intercostal nodes is present directly below the pleura in certain spaces, and these are supplemented by a scattering of nodes along the aorta (Figure 27-8). Both sets drain lymph from structures about the vertebral column and within the dorsal mediastinum. Most of their outflow is directed toward the cranial mediastinal nodes.Caudal sternal nodes are concealed below the transverse thoracic muscle on the thoracic floor, while a larger cranial sternal node lies in front of this. These nodes drain the ventral parts of the cranial abdominal and thoracic floors and also receive lymph from overlying muscles of the forelimbs. They direct their outflow to the cranial mediastinal group.
Other important nodes occupy more central positions. A cranial mediastinal group, scattered among various structures near the entrance to the thorax, drains the adjacent part of the mediastinum as well as the dorsal and ventral groups recently mentioned. The outflow goes to the thoracic duct or to one of the tracheal ducts. Middle mediastinal nodes lying to the right of the aortic arch receive lymph from adjacent structures and from a portion of the tracheobronchial nodes. The efferent flow passes in part directly to the thoracic duct, in part to the other mediastinal groups. The tracheobronchial nodes placed directly on the trachea and principal bronchi receive lymph from the lungs and distribute this among the various mediastinal nodes.
The caudal mediastinal group comprises only one or two nodes. The larger and possibly solitary node may
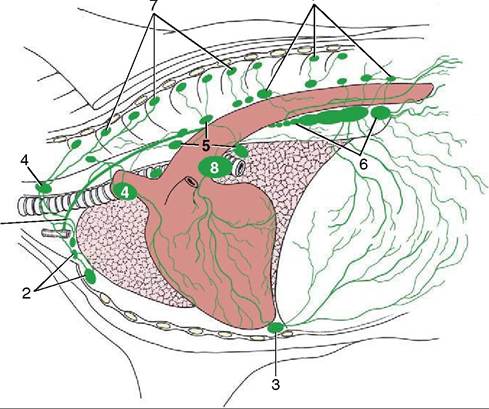
Figure 27-8 Lymph drainage of the bovine thoracic wall and mediastinum. 1, Thoracic duct; 2, cranial sternal lymph nodes; 3, caudal sternal lymph node; 4, cranial mediastinal lymph nodes; 5, middle mediastinal lymph nodes; 6, caudal mediastinal lymph nodes; 7, intercostal and thoracic aortic lymph nodes; 8, tracheobronchial node.
attain a length of 20 cm; it is flexed to fit over the diaphragm, dorsal to the hiatus, and over the terminal part of the esophagus. Pathological conditions in this node may cause it to press on the esophagus, which would impede the eructation of ruminal gas, or interfere with vagal control of gastric function.
The thoracic duct, into which most of the lymph eventually flows, inclines ventrally over the left face of the trachea to end by opening into the cranial vena cava or one of its tributaries of the left side. The duct is often duplicated for all or part of its course.