THE MAJOR NERVES OF THE FORELIMB
This account is concerned only with the nerves distal to the shoulder. Because the main features conform closely to the common pattern (pp. 321-323), it is sufficient to concentrate attention on their relations and cutaneous distribution.
The brachial plexus originates from C6-T1 in about 60%, from C5-T1 in 20%, from C6-T2 in about 20%, and from C5-T2 in a very small proportion (less than 3%) of dogs. The origins of the individual nerves are therefore subject to considerable variation; those described later refer to the most common arrangements. There is also considerable overlap between their cutaneous territories, which can be indicated only approximately. Figure 16-12 shows the much smaller autonomous zones used for testing the integrity of individual nerves. The courses and distributions of the nerves within the paw have little clinical application and can be dealt with summarily.The musculocutaneous nerve (C6-C7) innervates the biceps, brachialis, and coracobrachialis. It descends on the medial surface of the arm between the biceps and the brachial artery and, at the elbow, detaches a communicating branch to the more caudally placed median nerve. It is continued into the forearm by a cutaneous branch (medial cutaneous antebrachial nerve), which passes between the biceps and brachialis to become subcutaneous craniomedial to the elbow, before supply-

Figure 16-11 Dorsopalmar and lateral radiographic views of the canine (A and B) and feline (C and D) forepaws. E and F, Oblique and dorsopalmar views of feline digits; note how the distal phalanges slide next to the middle phalanges when the claws are retracted. 1, Radius; 2, ulna; 3, radial carpal; 4, ulnar carpal; 5, accessory carpal; 6, 6', third and fourth metacarpals; 7, metacarpal pad; 7, distal border of 7,8, a digital pad.
ing skin over the medial surface of the forearm (Figure 16—12/2 and Figure 16—13/7,77). Although dysfunction of the nerve causes little change in gait, an affected animal is unable to respond to the invitation to “offer a paw” because flexion of the elbow requires activity of at least one of the biceps and brachialis muscles.
The axillary nerve (C7-C8) supplies the prime flexors of the shoulder joint. It leaves the axillary space by disappearing dorsal to the teres major (Figure 16-2/4,5) and then winds around the caudal aspect of the joint to reach the deltoideus; the branches that continue beyond this point supply skin over the craniolateral region of the arm and a part of the forearm (Figure 16-12/7). Paralysis of the nerve has little effect because the latissimus dorsi and the long head of the triceps are available to compensate for the loss of most shoulder flexors.
The median nerve (C8-T1) innervates most flexors of the carpus and digits. It descends on the medial surface of the arm just caudal to the brachial artery and passes the elbow cranial to the medial collateral ligament before dipping under the pronator teres and flexor carpi radialis muscles (Figure 16-13/7). It detaches most muscular branches here and then continues (under cover of the last-named muscle) near the medial border of the
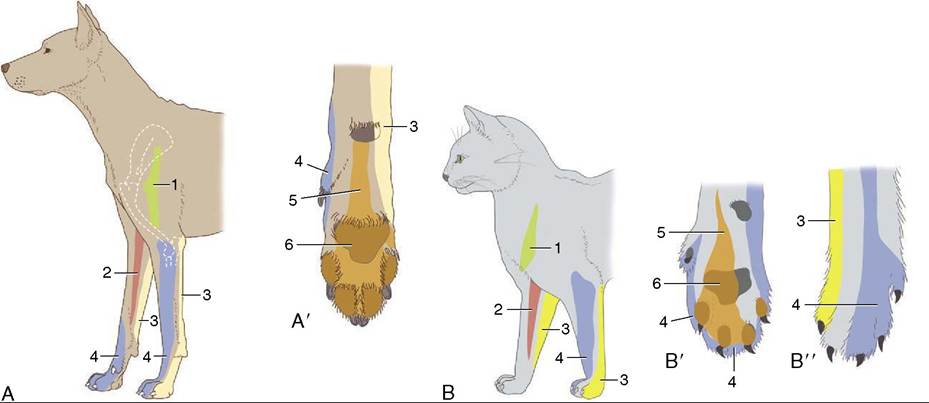
Figure 16-12 The autonomous zones of the cutaneous innervation of the canine (A, A') and feline (B, B', B") forelimb. 1, Axillary nerve (green); 2, musculocutaneous nerve (red); 3, ulnar nerve (yellow); 4, radial nerve (blue); 5, median nerve (orange); 6, mixture of median and ulnar nerves (brown).
radius as a mainly sensory nerve. This accompanies the digital flexor tendons and the median artery through the carpal canal before dividing to supply the medial and palmar aspects of the paw in collaboration with the ulnar nerve. Dysfunction has little effect on the gait, but the carpus may become overextended when the dog is standing, which results in the claws being slightly raised from their normal posture.
The ulnar nerve (C8-T1) innervates the remaining carpal and digital flexors. It first descends with the median nerve, but in the distal half of the arm it seeks a more caudal course, which takes it over the medial epicondyle of the humerus (where it is palpable) accompanied by the collateral ulnar vessels (Figure 16-13/d). A cutaneous branch (caudal cutaneous antebrachial nerve; Figure 16-13/5) that becomes subcutaneous on the medial aspect of the olecranon supplies the caudal surface of the forearm. The main trunk dives into the caudomedial forearm muscles, and after supplying some of these, it re-emerges on the lateral side, where it joins the ulnar artery and vein before descending caudal to the ulna. It divides into dorsal and palmar branches in the distal half of the forearm. The dorsal branch comes to the surface in the large depression between the ulnaris lateralis and the flexor carpi ulnaris and innervates the skin on the lateropalmar aspect of the paw. The palmar branch crosses the carpus with the flexor tendons and median nerve to supply the palmar aspect of the paw. Paralysis of the nerve has no obvious effect on gait or posture.
The important radial nerve (C7-T1) supplies the extensors of the elbow, carpal, and digital joints. It leaves the axilla by plunging into the triceps, about the middle of the arm (Figure 16-2/7). After detaching branches to the triceps, it accompanies the brachialis muscle around the lateral aspect of the humerus to gain the flexor surface of the elbow. In this part of its course, it is eminently vulnerable in fractures and from the tumors that commonly affect the humerus. It divides into deep and superficial branches before leaving the arm. The former continues distally, first between the brachialis and extensor carpi radialis and then between the supinator and the joint capsule, to supply the carpal and digital extensors in the upper part of the forearm. The latter splits into medial and lateral branches that emerge from the cranial border of the lateral head of the triceps to run subcutaneously, one to each side of the cephalic vein; they enter the paw with the accessory cephalic vein (Figure 16-4/7,7').
The superficial branch supplies skin on the dorsal surface of the forearm and paw, sharing the most proximal part of this region with the axillary nerve (Figure 16-12/4).If the nerve is seriously injured proximal to the origin of the tricipital branches, the elbow cannot be fixed, and the limb, unable to bear weight, is carried in the flexed position with the toes knuckled over and presenting their dorsal surfaces to the ground. More distal injury is less serious because the dog soon learns to compensate for loss of the digital extensors by flicking the raised paw forward so that it lands on the pads.
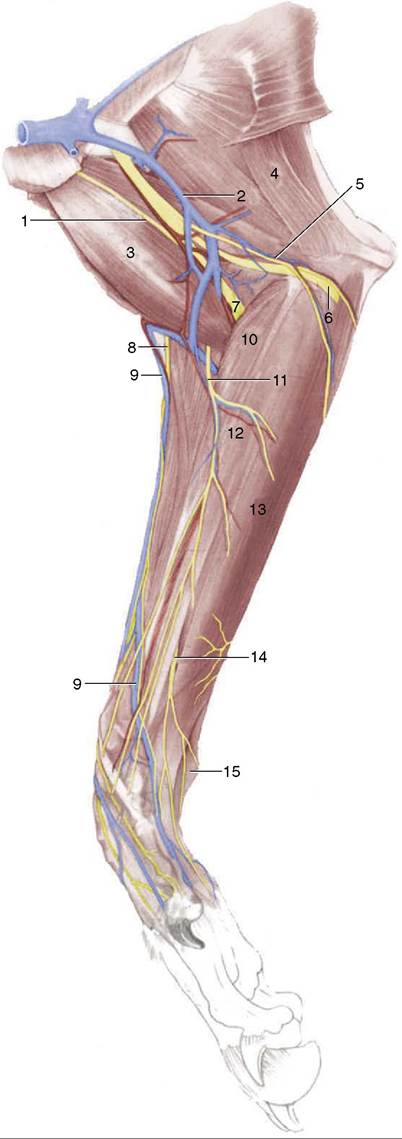
Figure 16-13 Superficial dissection of the right canine forelimb, medial view. 1, Musculocutaneous nerve; 2, brachial vein; 3, biceps; 4, tensor fasciae antebrachii; 5, caudal cutaneous antebrachial nerve and collateral ulnar vessels; 6, ulnar nerve; 7, median nerve and brachial artery; 8, medial branch of superficial radial nerve; 9, cephalic vein; 10, pronator teres; 11, medial cutaneous antebrachial nerve; 12, flexor carpi radialis; 13, superficial digital flexor; 14, inconstant cutaneous branch of ulnar nerve; 15, accessory carpal bone.