THE CROUP, HIP, AND THIGH
(See also pp. 88, 91, and 93-97.)
The habitual stance varies among breeds. The major differences are well illustrated by the German Shepherd, which tends to crouch with the back and croup sloping down toward the tail (and the hip, stifle, and hock joints markedly flexed), and the Boxer, which favors a stiffer, more upright posture (with the major joints, particularly the hock, significantly straighter).
The more upright limb appears to predispose to several common stifle disorders. In the Greyhound and other lean, short- coated dogs, the contours of the croup may reproduce the form of the underlying muscles, the superficial gluteal especially; however, such details are more often obscured by subcutaneous fat or a thick coat. The major skeletal landmarks are always palpable and reveal the small angle the ilium makes with the vertebral column.The dorsal and ventral spines of the ilium are very prominent. The convex (iliac) crest joining these points can also be followed in its length and provides a convenient site for bone marrow biopsy in larger breeds; it is too thin to serve this purpose in smaller animals. A narrow strip of the pelvic floor bordering the ischial arch can usually be palpated between the salient tubers. In the dog the cordlike sacrotuberous ligaments, which are lacking in cats, can also be felt as they approach these projections from their origins on the sacrum. The greater trochanter of the femur is found cranial to the ischial tuber, and because its summit is very nearly level with the femoral head, it provides a good guide to the position of the joint, which is not itself palpable. Attention should be paid to the spacing of these features of the ilium, ischium, and femur because alteration may reveal luxation of the femur. This is a relatively frequent mishap; the femoral head is most often displaced dor- socranially (which widens the ischiofemoral gap) but may pass dorsocaudally or, though rarely, ventrocau- dally when it may engage within the obturator foramen.
Luxation may be confirmed by rotating the thigh outward while the thumb is pressed between the trochanter and the tuber; the movement normally forces the thumb from the recess, but a luxated femur is unable to exert the necessary leverage.Although the hip joint is constructed according to the usual plan, it possesses greater range and versatility of movement in the dog and cat than in other domestic species. The enhanced potential for abduction is shown by the ease with which dogs cock their legs when urinating, while the general versatility, taken in combination with the suppleness of the trunk, enables both species to reach most parts of the head, neck, and thorax when scratching with the hindpaw. The articular surfaces reflect these abilities. The femoral head is an almost perfect hemisphere, marred only by the small central fovea where the intracapsular ligament (of the femoral head) inserts; it is deeply seated within the acetabular cup, which is only slightly extended by a labrum about its rim (see Figure 2-62). There are no peripheral ligaments to limit movement, although some capsule reinforcements can be identified. The intracapsular ligament, though variable in length and thickness, is generally lax enough to survive intact when the head is subluxated; this may be the case when there is preexisting dysplasia of the joint, as then the ligament is often hypertrophied. In normal hips, the ligament is thought to exert a braking function on movements that threaten the stability of the joint. The joint capsule also maintains the femoral head within the socket and prevents overextension and flexion. The fit of the femoral head within the acetabulum can be estimated from a ventrodorsal radiograph of the pelvis by measuring the “Norberg angle,” that is, the angle between the line connecting the centers of the femoral heads and that connecting the center of a femoral head with the cranial part of the related acetabular rim. An angle of less than 105° indicates displacement and suggests dysplasia.
The blood supply to the joint capsule, the femoral neck, and the proximal epiphysis arises from the lateral and medial circumflex femoral arteries, which, with some assistance from the caudal gluteal artery, form an extracapsular ring from which branches pierce the joint capsule. These ascend the femoral neck and provide the epiphyseal arteries of the head. Arteries demonstrable in the ligament of the femoral head are thought to be of little significance in the dog but make a major contribution to the supply of the femoral head of the kitten. Trauma to the femoral neck often leads to its absorption because of the limited blood supply.
The most convenient access to the joint, for puncture and in surgery, is from the craniolateral direction. An approach between the tensor and biceps muscles exposes the proximal part of the vastus lateralis (whose origin runs from just below the greater trochanter) and the gluteal muscles that clothe the joint directly. The important structures endangered are the sciatic nerve and the caudal gluteal vessels; however, because these cross the dorsocaudal aspect of the joint as they proceed into the thigh, the risk is relatively remote.
The radiological anatomy is very relevant to the diagnosis of the two conditions that commonly affect the joint: luxation and dysplasia. For the standard ventrodorsal radiograph (Figure 17-1, A) the supine animal must be placed with its hindlimbs drawn uniformly backward to ensure symmetrical depiction of bilateral structures. Although most features of the pelvis are too obvious to require comment, attention may be drawn to the slight lateral bowing of the canine ilia (in contrast to their parallel course in the cat). The relationship between the rim of the acetabulum and the femoral head on which it is superimposed is of the greatest importance in determining the integrity of the joint (Figure 17-1/5). Attention is also directed to the relative radiolucency of the region (corresponding to the trochanteric fossa) between the greater and lesser trochanters of the femur, as it is sometimes misinterpreted. The less useful lateral view reveals the position of the hip joints below the first two caudal vertebrae (Figure 17-1, D).
The maturation of the skeleton can be followed in radiographs obtained from young animals. In puppies there are primary ossification centers for the bodies of the ilium, ischium, and pubis and for the acetabular bone and secondary centers for the iliac crest, ischial tuber, and the border of the ischial arch. The acetabular bone is the first to lose its independence, but this is followed by the merger of the other primary centers at a comparatively early age (4 to 6 months); the secondary centers remain distinct until much later (15 months to 5 years for the iliac crest and 8 to 14 months for the ischial tuber). Fusion at the proximal extremity of the femur is completed between the 6th and 12th month (Table 17-1 and Figure 5-74).
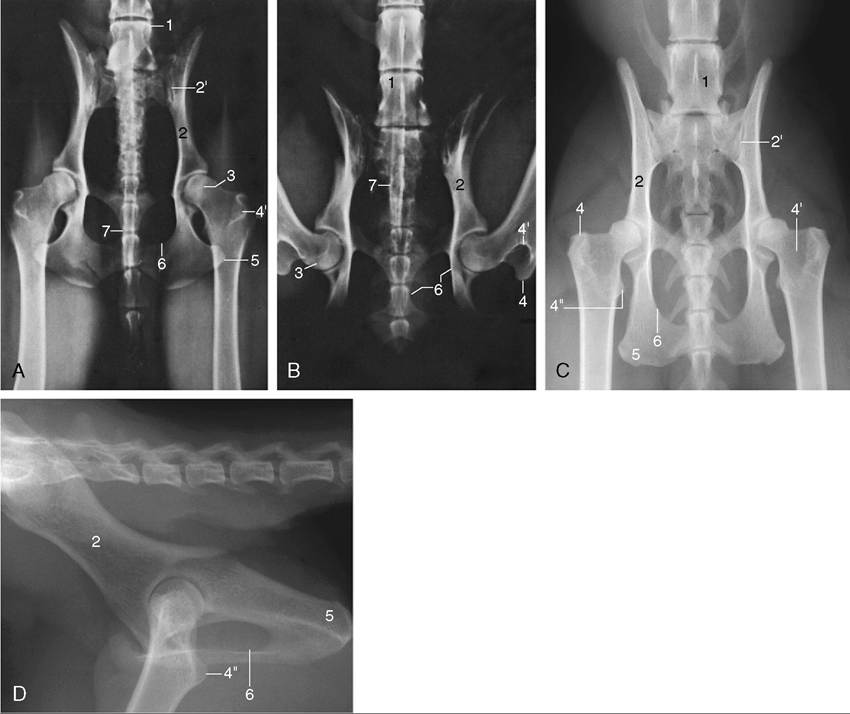
Figure 17-1 Ventrodorsal radiographic views of the canine pelvis with extended (A) and flexed (B) hip joints. C and D, Radiographs of the feline pelvis in ventrodorsal and lateral views; D is taken of a specimen. 1, Last lumbar vertebra (L7); 2, shaft of ilium; 2', sacroiliac joint; 3, dorsal border of acetabulum superimposed on the femoral head; 4, greater trochanter; 4', trochanteric fossa; 4", lesser trochanter; 5, ischial tuber; 6, obturator foramen; 7, os penis superimposed on vertebrae.
A special position, in which the hindlimbs of the supine animal are rotated inward until the femoral trochleae and patellae face directly upward, is used for the better depiction of the contours of the femoral head when hip dysplasia is suspected. In this view it is easier to gauge the congruence of the femoral head with the acetabulum and to recognize any flattening or distortion of its contours. Progressive deformation of the head and worsening of fit characterize the progress of the condition.
The etiology of hip dysplasia, very common in certain larger breeds and with a familial tendency, is uncertain. Several once promising theories have been abandoned, and much work has concentrated on the belief that the dysplasia, which inevitably leads to osteo- arthritic changes, is a consequence of the instability permitted by abnormally lax soft articular tissues.
It has been shown that many affected dogs exhibit similar but milder features of the capsules of certain other joints. This prompts the suspicion that the dysplasia is not so much a unique affection of the hip but a particularly severe local manifestation of a more widespread developmental disorder.The shaft of the femur is so deeply embedded among the muscles of the thigh that only a general impression of its presence may be obtained on palpation (Figure 17-2/9). Despite this protection, the femur is the most commonly fractured bone, and most breaks occur about or below midshaft level. Such fractures are often complicated by considerable overriding; the lower fragment is commonly displaced caudally by the pull of the gastrocnemius. They are often repaired by intramedullary pinning, a procedure usually requiring direct exposure of the break. A lateral approach is most convenient: after incision of the fascia lata, the biceps, whose cranial margin is often palpable through the skin, is reflected, which completes the exposure of the vastus lateralis; the path is now open to the bone along the attachment of the latter muscle (Figure 17-2/8,9,10).
Although the caudal thigh muscles appear to lend themselves to intramuscular injection, they should be avoided for this purpose because of possible damage to the sciatic nerve; a better alternative is injection into the muscles of the back.
The gluteal muscles have been described. Caudal to these, the cat presents the gluteofemoral, a long and relatively strong muscle that arises from the second to fourth caudal vertebrae and runs caudal to the superficial gluteal and cranial to the biceps to insert lateral to the patella in the fascia lata. It retracts the hindlimb and may also draw the tail to the side. The biceps femoris covers the abductor cruris caudalis, a small, thin muscle strap that emerges over the lateral head of the gastrocnemius in the lower leg.
The most important palpable structure of the thigh is the femoral artery (Figure 17-2/2), which is subcutaneous on the medial aspect of the limb toward the groin.
It lies within the femoral triangle, a pyramidal space whose base lies toward the vascular lacuna (the passage to and from the abdomen for the femoral artery and vein) and whose tip is closed distally by the convergence of the sartorius and pectineus muscles that form its cranial and caudal walls. The pectineus forms so obtrusive a fusiform swelling that it immediately guides the fingers to the adjacent artery, which is the first choice for the evaluation of the circulation. Pulsation may still be perceived in a stretch of the artery after it dives more deeply among the muscles of the thigh. Its course leads it across the medial aspect of the femur to reach the popliteal fossa, where it is renamed the popliteal artery (see Figure 17-6/1,2). The accompanying vein is less conspicuous, but its constant relationship to the caudal border of the artery makes it easily found and convenient for intravenous injection in the supine, anesthetized subject. The saphenous artery (see Figure 17-6/4) branches from the concealed part of the femoral but soon becomes subcutaneous and runs over the medial aspect of the thigh toward the stifle. Both it and a large, more proximal branch (running caudally toward the gracilis) may be palpated.Unlike the larger species, the dog and cat have no subiliac lymph nodes. However, the popliteal node is usually palpable within the popliteal fossa, between the distal parts of the biceps and semitendinosus as they diverge toward their insertions at the stifle (see Figure 17-3/10 and Figure 17-5/6).