The Muscles of the Trunk
The Cutaneous Muscle of the Trunk
The cutaneous muscle of the trunk (Fig. 2.21) varies in relative thickness and extent but generally covers the lateral aspect of the thorax and abdomen with fascicles with a predominately horizontal course.
Contained with the superficial fascia, it tenses and twitches the skin. In some animals, detachments are associated with the prepuce, and in horses and cattle a separate lamella covers the shoulder and arm regions. The innervation comes from the brachial plexus.The Muscles of the Vertebral Column
The muscles of the vertebral column can be separated into two divisions according to their position and innervation. The epaxial division (Fig. 2.22B/12) is dorsal to the line of the transverse processes of the vertebrae and receives its nerve supply from dorsal branches of the spinal nerves. The hypaxial division (Fig. 2.22/14), ventral to the transverse processes, is supplied by the ventral branches of these nerves. It includes the muscles of the thoracic and abdominal walls in addition to those placed closely on the vertebrae. The thoracic and abdominal muscles are considered in later sections.
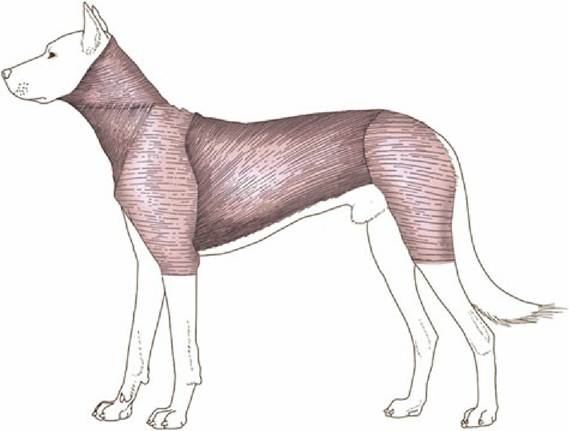
FIG. 2.21 The cutaneous muscle of the dog.
The Epaxial Muscles
Although numerous and complicated, the epaxial muscles fortunately do not require detailed description because they are rarely of clinical importance, except in the dog (p. 398). The major muscles are arranged in three parallel columns (Fig. 2.22C/19-21), which show some tendency to fuse over the loins and to split into additional units in the neck. They are extensors of the vertebral column, locally or more generally according to their extent, and are relatively more powerful in animals that make use of a bounding gait when traveling at speed (e.g., the dog).
The lateral column, the iliocostalis, arises from the ilium and transverse processes of the lumbar vertebrae and inserts on the more cranial lumbar vertebrae and ribs with, in most species, a weaker continuation into the neck. It is composed of many fascicles that overlap and generally span about four vertebrae. Its lateral position also makes this column effective in bending the trunk to the side (Fig. 2.23B/17).
The middle column, the longissimus (Fig. 2.23/16), is strongest and can be followed into the neck and even to the head. Some of its more cranial parts are independent to a greater or lesser degree. The caudal attachments, which are the conventional origin, are from the ilium, the sacrum, and the mammillary processes, whereas the insertions are to the transverse processes and ribs. The fascicles thus pursue a cranial, lateral, and ventral course, and each bridges several vertebrae; the longest fascicles span the especially mobile thoracolumbar junction. Different parts may be designated longissimus lumborum, longissimus dorsi, longissimus cervicis, longissimus atlantis, and longissimus capitis, but usually the generic term is sufficient. The muscle tends to fuse with its medial and lateral neighbors in the lumbar region.
In addition to the more or less direct continuation, the cervical part of the longissimus is closely associated with the more superficial splenius (Fig. 2.23A/4). This muscle passes from the highest spines of the withers and thoracolumbar fascia to the occipitomastoid region of the skull. It is covered by certain muscles of the thoracic girdle, especially the trapezius and rhomboideus.
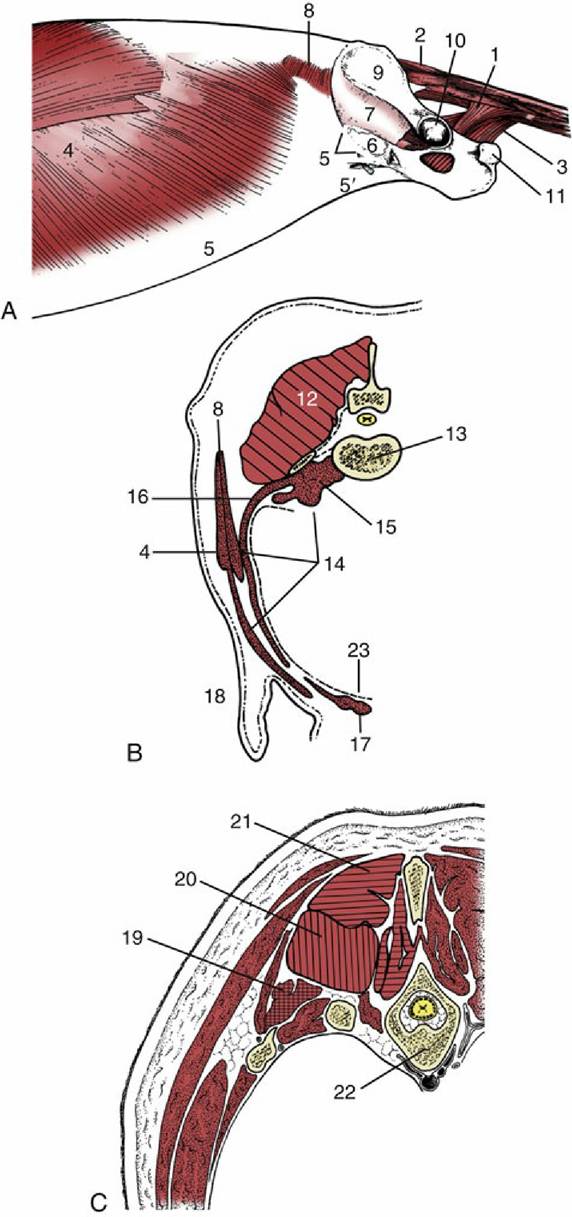
FIG. 2.22 (A) Trunk muscles of the dog, lateral view; the limbs have been removed. (B) Epaxial (hatched) and hypaxial (stippled) muscles shown in a transverse section of the lumbar region. (C) The three systems of epaxial muscles at the level of the thorax.
1, Coccygeus; 2, dorsal sacrocaudal; 3, levator ani; 4, external abdominal oblique; 5, its aponeurosis, pelvic tendon, and inguinal ligament; 5', abdominal tendon; 6, vascular lacuna; 7, iliopsoas; 8, internal abdominal oblique; 9, wing of ilium; 10, acetabulum; 11, ischial tuber; 12, epaxial muscles; 13, lumbar vertebra—its transverse process appears as detached section; 14, hypaxial muscles; 15, psoas muscles; 16, transverse abdominis; 17, rectus abdominis; 18, flank fold; 19, iliocostalis system (crosshatched); 20, longissimus system (vertically hatched); 21, transversospinalis system (horizontally hatched); 22, thoracic vertebra and ribs; 23, peritoneum.
FIG. 2.23 (A) and (B) Trunk muscles of the dog, deeper layers. 1, Longus capitis; 2, trachea; 3, esophagus; 4, splenius; 5, serratus dorsalis cranialis; 6, serratus caudalis; 7, internal abdominal oblique;
8, its aponeurosis; 9, rectus abdominis; 10, caudal free border of internal abdominal oblique; 11, cremaster; 12, inguinal ligament; 12', external abdominal oblique aponeurosis, cut and reflected; 13, fascia iliopsoas; 14, dorsal sacrocaudal muscles; 15, transversospinalis system; 15', semispinalis capitis; 15", spinalis et semispinalis; 16, longissimus system; 16', longissimus capitis and longissimus cervicis; 16", longissimus thoracis; 17, iliocostalis; 18, transversus abdominis; 19, transverse fascia.
The longissimus complex also includes certain small muscles passing between adjacent transverse processes as well as the dorsal (sacrocaudal) muscles of the tail (Fig. 2.23/14); the latter are fleshy at their origin and are continued by tendons that run the length of the tail.
The medial column, the transversospinalis system (Fig. 2.24/2), is the most complex, and the number of discrete subunits varies among species. It lies on and between the medial parts of the vertebral arches and the spinous processes.
Some fascicles run sagittally; others pursue a cranial, medial, and dorsal course from their caudal origin. The sagittal bundles include small units, often converted into ligaments, that pass between adjacent spinous processes as well as larger units that span several vertebrae. The oblique bundles run from mammillary to spinous processes and may be distinguished by name according to whether they span one, two, three, or more joints. The longest fascicles are again concentrated at the middle, most mobile region of the back.A number of specialized units bridge the joints between the axis, the atlas, and the skull and are responsible for the special movements in this region. Those of the dog are briefly described later (p. 398).
The Hypaxial Muscles
The hypaxial muscles are flexor muscles of the neck or tail. The longus colli (Fig. 2.24/9) runs from the cranial thoracic region to the atlas, covering the ventral surfaces of the vertebral bodies. It has a complex organization, and most of its constituent bundles of varying orientation are relatively short and cross only a few joints. It is complemented by the rectus capitis ventralis (Fig. 2.24/1), which extends from the atlas to the ventral aspect of the skull, and the longus capitis (Fig. 2.24/1), which lies lateral to the longus colli and extends from the transverse processes of the midcervical vertebrae to the skull. The scalenus group occupies a similar position in relation to the caudal cervical vertebrae. It passes to the first one or few ribs, which it helps stabilize during inspiration. In some species the scalenus is readily divisible into dorsal, middle, and ventral parts.
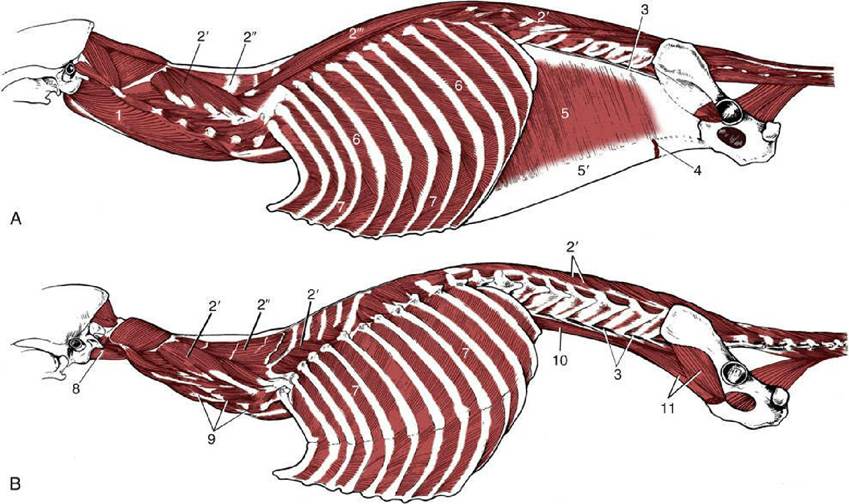
FIG. 2.24 (A) and (B) Trunk muscles of the dog, deepest layers. 1, Longus capitis; 2, transversospinalis system; 2', multifidus; 2", spinalis cervicis; 2'", spinalis et semispinalis; 3, quadratus lumborum; 4, rectus abdominis; 5, transversus abdominis; 5', its aponeurosis; 6, external intercostal muscles; 7, internal intercostal muscles; 8, rectus capitis ventralis; 9, longus colli; 10, psoas minor; 11, iliopsoas (psoas major and iliacus).
The ventral muscles of the tail are close counterparts of the dorsal muscles.
The Muscles of the Thoracic Wall
The muscles of the thoracic wall are primarily concerned with respiration. Most are inspiratory and enlarge the thoracic cavity, causing air to flow into the lungs. Some are expiratory and diminish the cavity, expelling air. They comprise muscles that fill the spaces between the ribs, certain small units placed lateral to the ribs, and, by far the most important, the diaphragm.
The intercostal muscles are theoretically arranged in three layers that correspond to the layers of the abdominal wall. The external intercostal muscles are outermost (Fig. 2.24/6). Each of these muscles is confined to a single intercostal space in which its fibers run caudoventrally from one rib to the following rib. They fill the spaces from the upper ends to the costochondral junctions and sometimes beyond them but fail to reach the sternum. The parts between the cartilages are sometimes separately named. The internal intercostal muscles (Fig. 2.24/7) are placed more deeply within the intercostal spaces and run cranioventrally, approximately perpendicular to the course of the external muscles. They do not occupy the most dorsal parts of the spaces but do reach the margin of the sternum. The third (subcostal) layer is so weak and so inconsistently developed that it may be ignored. The transversus thoracis is a triangular sheet that arises from and covers the dorsal surface of the sternum. The apex points cranially, and the muscle splits into slips that run caudolaterally to insert on the sternal ribs close to the costochondral junctions. It is morphologically the equivalent of the ventral part of the transversus abdominis.
Two muscles lie on the lateral surface of the thoracic wall. The rectus thoracis is a small quadrilateral sheet placed over the lower ends of the first four ribs in apparent continuation of the rectus abdominis. The serratus dorsalis (Fig. 2.23A/5 and 6) lies over the dorsal parts of the ribs.
It takes origin from the fascia of the back and inserts on the ribs by a series of slips. The slips of the cranial part of the muscle slope caudoventrally, and those of the caudal part slope cranioventrally, a difference that points to antagonistic functions. The two parts are sometimes quite widely separated. The scalenus, mentioned in the preceding section, has an attachment to the first rib; in some species it also passes quite extensively over the rib cage.The diaphragm separates the thoracic and abdominal cavities. It is dome-shaped, being convex in all directions on its cranial surface, and bulges cranially under cover of the ribs to enlarge the abdomen at the expense of the thoracic cavity (Figs. 2.2 and 2.25A). It consists of a heart-shaped (trefoil-shaped in the dog) central tendon (Fig. 2.25/7) and a muscular periphery that is divisible into portions that arise from the lumbar vertebrae, the caudal ribs, and the sternum.
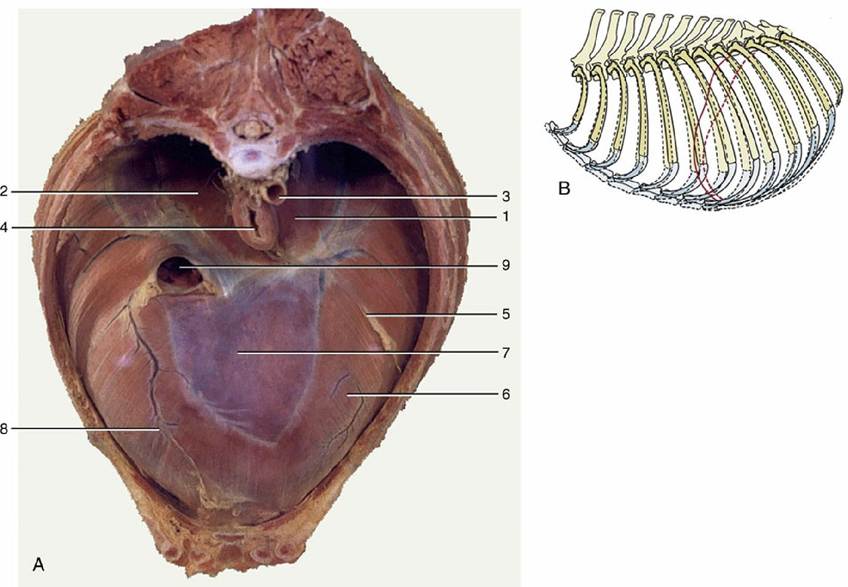
FIG. 2.25 A, Cranial view, preserved specimen, of the canine diaphragm. 1, Left crus; 2, right crus; 3, aorta; 4, esophagus; 5, attachment of caudal mediastinum to diaphragm; 6, sternal and costal parts of diaphragm; 7, tendinous center; 8, attachment of plica venae cavae; 9, caudal vena cava. (B) Lateral view diagram of the canine thorax showing ribs and cranial extent of diaphragm in inspiration (broken lines) and expiration (solid lines).
The central tendon, the most cranial part, forms the vertex. In the neutral position between full inspiration and full expiration, this tendon reaches the level of the lower part of the sixth rib (or following space) and is thus only a little behind the plane of the olecranon in an animal standing square. Knowledge of this fact and of the line of the costal attachment is indispensable in appreciating the extent of the thoracic cavity (Fig. 2.25B).
The powerful lumbar portion of the peripheral muscle consists of left and right crura (Fig. 2.25/1 and 2) that arise from the ventral aspect of the first three or four lumbar vertebrae by means of stout tendons. The right crus is considerably the larger, and it divides into three branches that radiate ventrally to join the central tendon. The left crus is undivided.
The origin of the thinner costal part is from the inner surfaces of the ribs and costal cartilages. Although the most caudal, also most dorsal slip, arises close to the dorsal end of the last rib, the cranial slips arise at successively more ventral levels with the last costal digitation following the cartilage of the eighth rib to the sternum. A final sternal slip arises from the dorsal surface of the sternum and runs dorsally to meet the tendon, which is thus bordered by muscle on all sides.
The diaphragm has three openings called the aortic hiatus, the esophageal hiatus, and the caval foramen (Fig. 2.25). These diaphragmatic openings transmit various structures.
The diaphragm is supplied by the phrenic nerves formed from contributions by ventral branches of caudal cervical nerves (usually C5-C7). Despite the apparently involuntary nature of breathing, the phrenic nerves are ordinary somatic nerves of mixed composition. The other muscles of the chest wall are supplied by intercostal nerves (ventral branches of thoracic spinal nerves).
Functional Considerations
The form and construction of the thorax represent a compromise between the requirements of posture and locomotion and the more specialized needs of respiration. In most domestic mammals the advantages of a barrel-shaped thorax for respiration are largely sacrificed to the easier movement allowed to the scapulae by flattening of the cranial part of the rib cage. The potential for movement of the cranial ribs is also reduced in favor of the more rigid construction that provides a stable origin for the muscles that pass between the trunk and the forelimbs.
Respiration causes changes in the form of the caudal part of the rib cage and abdomen. All species exhibit both costal and abdominal (i.e., diaphragmatic) modes of breathing, but their relative importance varies with the species, with the prevailing circumstances, and with the individual. It is certainly safe to conclude that normal respiration is always accompanied by contraction of the diaphragm, whereas involvement of the intercostal and other accessory respiratory muscles is less certain.
The diaphragm contracts against the resistance of the abdominal viscera, which must be displaced caudally into space provided by relaxation of the abdominal floor and flanks. In the course of this movement the central part of the dome of the diaphragm shifts backward, perhaps half a vertebral length in quiet breathing, while additional thoracic enlargement is obtained through flattening of diaphragm's peripheral parts. The attachment of liver to diaphragm also acts as a piston during fast locomotion to flatten parts of the caudal lobes of the lungs. Contraction of the sternocostal parts of the diaphragm, which attach to the last ribs, tends to pull these ribs inward in opposition to the outward and forward pull exerted on them by the intercostal muscles. It is a common observation (easily confirmed by watching a sleeping dog) that the last rib may actually be tucked inward during inspiration while its more cranial fellows move outward to broaden the thorax.
The actual movements undertaken by the ribs and the forces that produce them are controversial. The caudal inclination of the lower part of the rib (before it is turned forward by the cartilage) results in a movement by the rib that is compared to raising a bucket handle. Although there is dispute regarding the mechanisms of engagement of articular surfaces during rib movement, it is clear that the overall effect is to widen while shortening the rib cage. In humans and some quadrupeds (including the dog), a concurrent ventral displacement of the sternum occurs.
A considerable number of the muscles attaching to the ribs and sternum appear from their geometry to be capable of producing the necessary movements. However, human studies show that little of this potential is actually employed in quiet breathing. During inspiration the external intercostals and the interchondral parts of the internal intercostals are most consistently engaged. The scalenus (and possibly also muscles that pass forward from the manubrium) may assist in fixing the thoracic inlet. Expiration is mainly passive, and the elastic recoil of the lungs is the major force. The muscles of the abdominal wall may contract to reinforce the passive tension in the tendinous parts that raises the viscera and that indirectly helps to restore the diaphragm to its former position. Sometimes the deeper layer of intercostal muscle—the interosseous parts of the internal intercostals and the transversus thoracis—is also engaged.
Contrary to common belief, the diaphragm is not indispensable. Evidence obtained from experimental and clinical subjects (dogs and ruminants) shows that section or paralysis of both phrenic nerves caused little obvious loss of respiratory efficiency even under moderate stress. This evidence of course does not deny the diaphragm the major role in normal animals but does confirm both the presence of an ample reserve of inspiratory muscle and the role of the mechanical function of the abdominal viscera in respiration.
The Muscles of the Abdominal Wall
The muscles of the abdominal wall are conveniently divided into ventrolateral and dorsal (sublumbar) groups (Fig. 2.22B). The first comprises the muscles of the flanks and abdominal floor, which are important because they are incised in almost all surgical approaches to the abdomen. Most muscles of the second group properly belong to the girdle division of hindlimb musculature. They are included here because they constitute part of the body wall—namely, the roof of the abdomen to each side of the vertebral column.
The Ventrolateral Group
The intrinsic musculature of the flank comprises three broad fleshy sheets superimposed on each other with contrasting orientation of their fibers. Each is continued ventrally by an aponeurotic tendon that principally inserts within a fibrous cord, the linea alba, which runs in the ventral midline from the xiphoid cartilage to the cranial end of the pelvic symphysis (via the prepubic tendon). In so doing, the tendons ensheath the fourth muscle, the rectus abdominis, which pursues a sagittal course within the abdominal floor directly to the side of the linea alba. The following account is of the basic arrangement. The details vary among species and may have surgical importance, especially in the small species (Fig. 2.26; see also pp. 419-420).
The outermost external abdominal oblique muscle (Fig. 2.22/4) arises from the lateral surfaces of the ribs and from the lumbar fascia. The majority of its fibers runs caudoventrally, but the most dorsal bundles follow a more horizontal course. The aponeurosis (Fig. 2.22/5) that succeeds the fleshy part divides into two parts (tendons) before its insertion. The larger abdominal tendon terminates on the linea alba after passing ventral to the rectus muscle; the smaller pelvic tendon proceeds to attach on the fascia over the iliopsoas and on the pubic brim lateral to the insertion of the rectus (Fig. 2.27/3' and 4).
The second muscle, the internal abdominal oblique (Fig. 2.23/7), arises mainly from the coxal tuber (or the equivalent region of the ilium) but to lesser extents from the insertion of the pelvic tendon of the external oblique, the thoracolumbar fascia, and the tips of the lumbar transverse processes. This muscle fans out more obviously: its most caudal fascicles pass ventrocaudally, and although the next group runs more or less transversely in the plane of the coxal tuber, most pass ventrocranially. Some cranial fascicles insert directly on the last rib, but the bulk are continued by an aponeurosis (Fig. 2.23/8) that passes ventral to the rectus to reach the linea alba. Toward the midline some interchange of fibers between the aponeuroses of the two oblique muscles usually occurs. The origin from the pelvic tendon allows the muscle a free caudal edge (Fig. 2.23/10), which is mentioned again shortly in connection with the inguinal canal. A caudal slip (cremaster; Fig. 2.23/11) detached from the internal oblique passes onto the spermatic cord (p. 179).
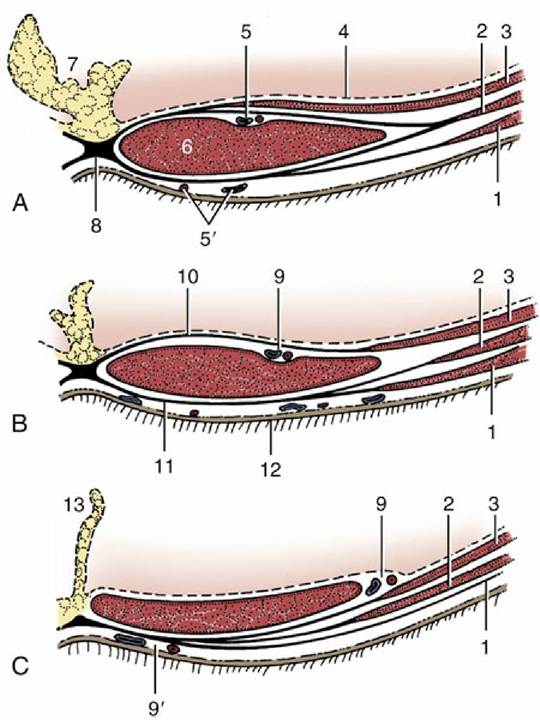
FIG. 2.26 Rectus sheath of the dog in transverse sections from (A) cranial and (B) caudal to the umbilicus and (C) near the pubis. 1, External abdominal oblique; 2, internal abdominal oblique; 3, transversus abdominis; 4, peritoneum; 5, cranial epigastric vessels; 5', cranial superficial epigastric
vessels; 6, rectus abdominis; 7, fat-filled falciform ligament; 8, linea alba; 9, caudal epigastric vessels; 9', caudal superficial epigastric vessels; 10, internal lamina of rectus sheath; 11, external lamina of rectus sheath; 12, skin; 13, median ligament of the bladder.
The deepest muscle of the flank, the transversus abdominis (Fig. 2.24/5), arises from the inner surfaces of the last ribs and the transverse processes of the lumbar vertebrae. Its fibers run more or less transversely and are succeeded by an aponeurosis (Fig. 2.24/5') that passes dorsal to the rectus abdominis before terminating on the linea alba. This muscle does not extend caudal to the coxal tuber. The caudal part of the tendon passes ventral to the rectus so that the most caudal part of that muscle is left uncovered dorsally.
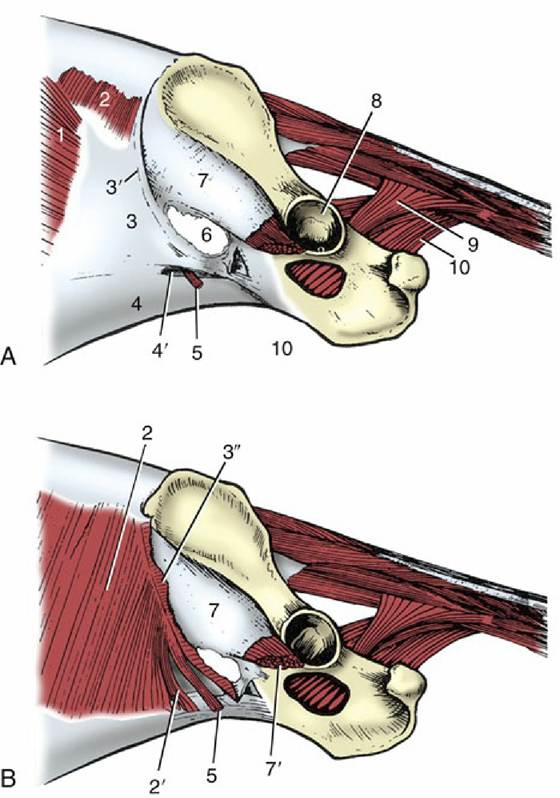
FIG. 2.27 Inguinal canal and pelvic diaphragm of the dog, left lateral view. The external abdominal oblique muscle, present in A, has been removed in B. 1, External abdominal oblique; 2, internal abdominal oblique; 2', free caudal edge of internal oblique, forming border of deep inguinal ring; 3, pelvic tendon of external oblique aponeurosis; 3', caudal border of 3 (inguinal ligament) ending on 7; 3", stump of external oblique aponeurosis reflected caudally (B); 4, abdominal tendon of external oblique aponeurosis; 4', superficial inguinal ring; 5, cremaster derived from internal oblique; 6, vascular lacuna; 7, iliac fascia covering iliopsoas; 7', iliopsoas; 8, acetabulum; 9, coccygeus; 10, levator ani.
The fourth muscle, the rectus abdominis (Fig. 2.23/9), forms a broad band to the side of the linea alba in the abdominal floor. It arises from the ventral surfaces of the rib cartilages and sternum and inserts on the pubic brim by means of a prepubic tendon. The fleshy part, which is widest about the middle of the abdomen, is divided into a series of segments by irregular transverse septa (tendinous intersections) that recall its polysegmental origin. The prepubic tendon serves as a common insertion for the abdominal muscles and the linea alba and may incorporate part of the tendons of origin of adductor (pectineus and gracilis) muscles of the thigh.
The rectus sheath (vagina musculi recti abdominis), the arrangement of the aponeurotic tendons of the flank muscles about the rectus abdominis, varies in detail among species. In the basic arrangement, the tendons of the two oblique muscles form a layer on the external (ventral) surface of the rectus, whereas that of the transversus lies against the internal surface; both layers merge with the linea alba to complete the enclosure (see Fig. 2.26 and p. 420).
The abdominal wall is perforated in the region of the groin by the inguinal canal (Figs. 2.27 and 21.5). Before or shortly after birth this canal transmits the testis in its descent toward the scrotum. In the adult male it contains the spermatic cord, consisting of the duct from the testis, and associated structures within an outpouching of the peritoneum. In both sexes, it also transmits the external pudendal artery and (usually) vein, efferent vessels from the superficial inguinal lymph nodes, and the genitofemoral nerve, all structures associated with the groin.
The term canal is misleading because it suggests a roomier passage than actually exists. The canal is a potential flat space between the fleshy part of the internal oblique on the one side and the pelvic tendon of the external oblique aponeurosis on the other (Fig. 2.27/2 and 3). The walls are apposed and joined by areolar tissue except where the transmitted structures hold them apart. The slitlike abdominal entrance to the canal (the deep inguinal ring) lies along the free caudal edge of the internal oblique muscle (Fig. 2.27/2'). The exit from the canal (the superficial inguinal ring; Fig. 2.27/4') is contained between the two divisions of the external oblique tendon. (The edges of the superficial inguinal ring are known as medial and lateral crura.) Species differences are mentioned in later chapters and may be of great importance because some explain why the escape of organs into and through the canal (inguinal hernia) occurs more readily in certain animals. Other differences are of immediate relevance to surgery in this area, most obviously in connection with castration, whether of the normal male or of one in which the testis has failed to descend and remains hidden within the abdomen or within the canal itself (cryptorchidism).
Functional Considerations
Observation and palpation suggest that animals standing quietly make little active use of the abdominal muscles in support of the viscera; the support is obtained from passive tension. Some electromyographic studies have revealed slight though continuous activity in the internal oblique and sporadic bursts in other muscles of the flank. Greater, and more pronounced in labored breathing, activity of the abdominal muscles may occur toward the end of quiet expiration to assist the forward recovery of the diaphragm.
When the abdominal muscles are contracted against a fixed diaphragm, the animal is said to "strain." The resulting increase in intraabdominal pressure reinforces the efforts of visceral muscle to expel urine, feces, or a fetus. The use made of straining varies with the species and conditions. Those animals that adopt a squatting posture for micturition (e.g., goat) or defecation (e.g., dog) obviously make more use of the abdominal muscles to assist expulsion.
The rigidity of the abdominal wall produced by contraction of these muscles may be used to protect the viscera during palpation in an animal with abdominal visceral pain. This defense is used by a nervous dog when efforts, particularly if unskillful, are made to palpate its abdomen; gentle massage may be necessary to allay the fear before the muscles relax.
These muscles are also used in the adjustment of posture and in progression. Acting unilaterally, the muscles of the flank bend the trunk to that side. Acting bilaterally, they may assist in arching the back, which is a movement of great importance in bounding gaits.
The ventrolateral abdominal muscles are supplied by caudal intercostal nerves and the ventral branches of the lumbar nerves, particularly those more cranial in the series.
The Sublumbar Muscles
The psoas minor (Fig. 2.24/10) arises from the bodies of the thoracolumbar vertebrae and inserts on the psoas minor tubercle on the ilium. Much tendon is intermingled in the flesh, supporting the contention that the muscle is probably employed mainly to stabilize the vertebral column. It may also rotate the pelvis at the sacroiliac joint.
The psoas major and iliacus muscles may be regarded as vertebral and pelvic heads of a single muscle (iliopsoas; Fig. 2.24/11) that terminates on the lesser trochanter of the femur. The psoas major arises from the bodies and ventral surfaces of the transverse processes of the lumbar vertebrae lateral to the psoas minor. The iliacus arises from the ventral aspect of the wing and shaft
of the ilium. The tendons of the two heads combine shortly before insertion. The iliopsoas is a flexor of the hip and an outward rotator of the thigh. The psoas head probably also contributes to the stability of the vertebral column.
The quadratus lumborum (Fig. 2.24/3) arises from the last ribs and from the transverse processes of the lumbar vertebrae and inserts on the wing of the sacrum (sometimes also on the ilium). It stabilizes the lumbar portion of the vertebral column.
These muscles are principally innervated by direct twigs from the ventral branches of the last few thoracic and the lumbar nerves. Other twigs detach from named branches of the lumbosacral plexus, principally the femoral nerve.
The Muscles of the Pelvic Outlet
The pelvic outlet is closed about the terminal parts of the digestive and urogenital tracts by a portion of the body wall known as the perineum. The projection of the perineum on the skin outlines the perineal region, the principal features of which are the anus and the vulva (in the female, to which we principally refer here). Because the ventral part of the vulva falls below the level of the pelvic floor, it is usual to enlarge the concept of the perineal region to embrace the whole vulva. Very often the dorsocaudal part of the udder (in animals such as the cow) is also included. Several muscles and fasciae interlace in a node between the anus and the vulva and vestibule, and this formation is properly known as the perineal body or center; however, in clinical, especially obstetric, literature the perineal body is frequently known simply, though incorrectly, as "the perineum." The three concepts—perineum, perineal region, and perineal body—should be kept distinct. Another potential source of confusion exists. In human anatomy, the structures that occupy the pelvic outlet are said to form a "floor" to the pelvic cavity. In quadrupeds, the "floor" is provided by the pelvic girdle. The difference in posture not only affects the appropriate use of vernacular terms but, more important, also modifies the function of homologous structures. The principal component of the dorsal part of the perineum is the pelvic diaphragm, an arrangement of striated muscles contained between fasciae, which closes about the anorectal junction. A similar but less conspicuous arrangement in the ventral part of the perineum, the urogenital diaphragm, closes about the vestibule.
The pelvic diaphragm attaches laterally to the pelvic wall and spreads caudomedially to close about the anal canal. The term diaphragm aptly describes the human arrangement, which forms a basin in which the pelvic organs rest. It is less appropriate in domestic species, in which the "halves" of the diaphragm have more sagittal courses and converge more gently on the anus, as a result of the relatively greater length of the pelvic girdle.
The more lateral of the two muscles of the diaphragm, the coccygeus (Fig. 2.27/9), is essentially a muscle of the tail. Rhomboidal in outline, it arises from the ischial spine, crosses the sacrotuberous ligament medially, and inserts on and about the transverse processes of the first few tail vertebrae.
The medial, thinner, and more extensive muscle, the levator ani, runs more obliquely in a dorsocaudal direction and is only partly covered by the coccygeus. The two muscles arise close together or by a common tendon in ungulates. In the dog, the levator has a more widely spread origin that continues from the iliac shaft over the cranial ramus of the pubis to follow the pelvic symphysis (Fig. 2.27/10). The insertion is divided between the fascia and vertebrae of the tail (extending distal to the insertion of the coccygeus) and the fascia about the anus and external anal sphincter. The tail attachment predominates in carnivores, the anal one in ungulates, in which considerable exchange of fascicles with the anal sphincter and constrictor vestibuli muscles occurs.
The coccygeus flexes the tail laterally or, when acting in concert with its fellow, draws the tail ventrally to cover the perineum, an attitude familiar in the nervous dog. The action of the levator is best known from an electromyographic study in the goat, and it is possible that important species differences exist. In the goat the muscle is active whenever the intra-abdominal pressure is raised, presumably to oppose the tendency to displace pelvic organs caudally. Although also involved in other visceral functions, it has a very definite relationship to defecation; it is active before the event (when it may fix the position of the anus against the contraction of the smooth muscle of the colon), becomes inactive during the event, and regains activity following the event (when it may restore the parts to their resting positions). The jerky movements of the dog's tail after defecation are probably evidence of levator activity in this species. Both muscles are supplied by ventral branches of the sacral nerves.
The smaller urogenital diaphragm (membrana perinei) contains more slender muscles, which are more appropriately described later with the reproductive organs. The fascia of the urogenital diaphragm attaches to the ischial arch and curves cranially, dorsally, and medially to blend with the ventral edge of the pelvic diaphragm and embrace the vestibule. It helps anchor the reproductive tract against a forward drag when the pregnant uterus sinks within the abdomen and against a backward displacement during parturition.
It may now be evident that to each side there is a space that is enclosed by the pelvic girdle but is excluded from the pelvic cavity by the pelvic diaphragm. This space is pyramidal and has a cranial apex, a lateral wall furnished by the ischial tuber and sacrotuberous ligament, a medial wall furnished by the pelvic diaphragm, a ventral wall furnished by the pelvic floor, and a base directed toward the skin. Appropriately known as the ischiorectal fossa, this space is normally occupied by fat (see Fig. 29.10/12). When this fat is depleted, a pronounced sinking of the skin to the side of the anus is apparent (except in the horse and pig, in which the vertebral head of the semimembranosus covers the region).