THE NASAL CAVITY AND PARANASAL SINUSES
The nasal cavity is much smaller than would be supposed from the exterior because its walls are widened and hollowed by air sinuses, while much of the internal space is occupied by the conchae.
Caudally, the nasal septum fails to reach the floor, which results in the formation of a single median channel that continues the paired nasal passages into the nasopharynx (Figures 25-9 and 25-10).Each nasal passage is divided by the major conchae into dorsal, middle, and ventral meatuses that branch from the common meatus located against the nasal septum. The deeper part of the cavity is further subdi-
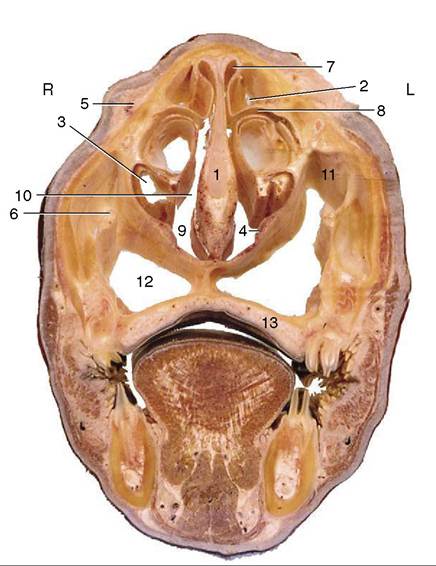
Figure 25-10 Transverse section of a bovine head at the level of the last premolars. 1, Nasal septum; 2, dorsal nasal concha; 3, ventral nasal concha; 4, thick nasal mucosa containing venous plexus; 5, nasolacrimal duct; 6, infraorbital canal with infraorbital nerve; 7, dorsal nasal meatus; 8, middle nasal meatus; 9, ventral nasal meatus; 10, common nasal meatus; 11, maxillary sinus; 12, palatine sinus; 13, hard palate.
vided by the numerous ethmoidal conchae; the largest of these projects rostrally and is known as the middle concha. The dorsal meatus leads to the ethmoidal meatuses; the middle meatus communicates with certain sinuses; and the ventral meatus is the principal respiratory pathway. The nasal route is occasionally chosen for the passage of a sound when the instrument is directed to follow the largest space, formed at the junction of the ventral and common meatuses (Figure 25-10/9).
The wall of each nasal passage is clothed by a thick, generously vascularized mucous membrane that ventrally encloses the vomeronasal organ.
The paranasal sinus system is very poorly developed in the young calf, and several years must elapse before it attains full size.
Even in the mature animal, the maxillary compartment continues to adjust to extrusion of the cheek teeth (Figures 25-3/1,5 and 25-11).The complete set of sinuses is very complicated. It comprises frontal compartments within the bones of the cranial roof and side walls; a palatomaxillary complex within the caudal part of the hard palate and the face, both before and below the orbit; a lacrimal
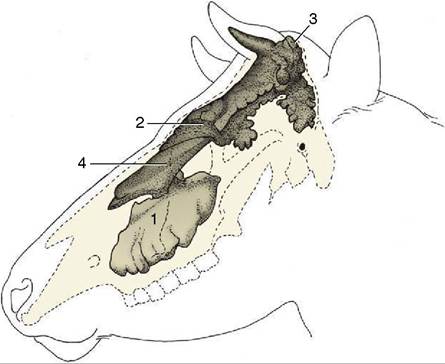
Figure 25-11 Topography of the paranasal sinuses, which are filled with casting material. 1, Maxillary sinus; 2, rostral frontal sinuses; 3, caudal frontal sinus; 4, dorsal conchal sinus.
sinus within the medial orbital wall; sphenoidal sinuses that extend past the orbit into the rostral part of the cranial floor; and conchal sinuses within the nasal conchae. Any of these may be infected or otherwise become an object of clinical interest, but in practice attention is concentrated on the maxillary and caudal frontal sinuses. The surface projections over which these spaces may be percussed are illustrated in Figures 25-11 and 25-12.
The maxillary sinus occupies much of the upper jaw above the alveoli of the cheek teeth. It communicates with the nasal cavity via a large nasomaxillary opening, but natural drainage of pus or other fluid is hindered by the location of this opening high in the medial wall. The maxillary sinus is continuous with the palatine sinus over the plate of bone that carries the infraorbital nerve in its free margin (Figure 25-10/d). It also extends caudally (as the lacrimal sinus in front of the orbit) and within the fragile lacrimal bulla that intrudes into the ventral part of the orbit.
The frontal sinus comprises several compartments that communicate separately with ethmoidal meatuses. The two or, occasionally, three small rostral compartments are of little clinical interest. The caudal compartment, by far the largest and most important, spreads mainly within the frontal bone.
It covers the dorsal part of the brain case and also extends into the lateral and nuchal walls and into the horn core. It is separated from its fellow and from the smaller ipsilateral compartments by partitions of rather variable position (Figure 25-12). The openings in these partitions, visible in dry skulls, are closed by mucosa in the fresh state. The major cavity, which continues to increase throughout life, is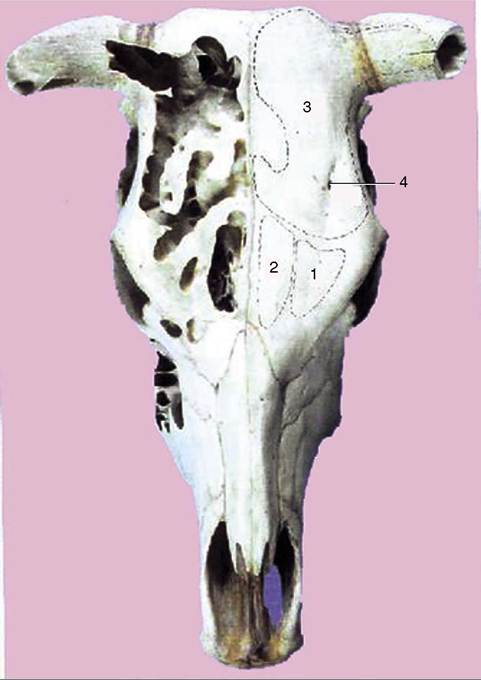
Figure 25-12 Dorsal projection of the frontal sinuses. 1, Lateral rostral frontal sinus; 2, medial rostral frontal sinus; 3, caudal frontal sinus with cornual diverticulum; 4, supraorbital foramen.
further subdivided by irregular and perforate septa. Inflammation of its mucosa is a common sequel to surgical dehorning.
The protection that the frontal sinus affords the cranial cavity makes it impossible to predict the extent of the latter by simple inspection of the head. The cranial cavity is in fact surprisingly small, rather globular, and so tilted that its rostral extremity is placed above as well as behind the nasal cavity (Figure 25-9). It is protected above, behind, and to the sides by the pneumatized bones of the cranial vault. The topography is relevant to the usual humane slaughter technique. The target spot is defined by the intersection of the diagonals joining the lateral angles of the eyes to the nearest parts of the opposite horn bases (or equivalent points in polled breeds). The bolt or bullet then has to pass through the shallowest part of the frontal sinus en route to the brain.
The maxillary sinus is shallower and simpler in the sheep and goat. It does not communicate with the lac-
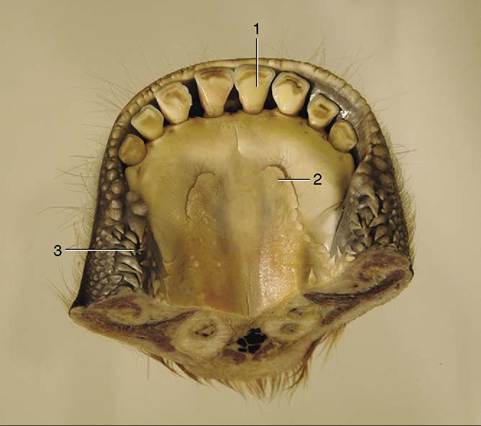
Figure 25-13 Floor of the bovine mouth. 1, Central incisor;
2, sublingual caruncle; 3, buccal papillae.
rimal sinus, which may open into the nasal cavity separately or via the lateral frontal sinus. The frontal sinus comprises separate medial and lateral compartments in both these species. They lie medial to the orbit (and extend slightly beyond this, both rostrally and caudally) and are of irregular form. The lateral compartment corresponds to the caudal sinus of cattle and provides the extension into the horn core.
The most common clinical involvement of the sinuses of sheep is that caused by invasion of the frontal sinus by larvae of oestrid flies. Treatment involves surgical puncture, and the preferred sites are rostral to the horn or medial to the middle of the orbital rim, where there is no risk of injury to the frontal vein.