THE PLEURAL CAVITIES
The arrangement of the pleura follows the usual pattern in that the thoracic interior is divided into two pleural
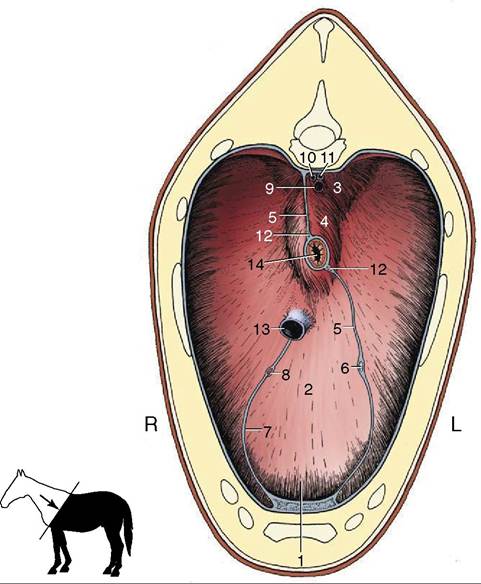
Figure 20-4 Cranial surface of the diaphragm.
1, Sternal and costal parts of diaphragm; 2, tendinous center; 3, left crus; 4, right crus; 5, caudal mediastinum; 6, left phrenic nerve; 7, plica venae cavae; 8, right phrenic nerve; 9, aorta; 10, right azygous vein; 11, thoracic duct; 12, dorsal and ventral vagal trunks; 13, caudal vena cava; 14, esophagus.cavities by an intermediate septum, the mediastinum. The subpleural connective tissue is poorly developed; as a result, the mediastinum is weak.
The projection of the pleural cavities on the chest wall is always a matter of clinical significance. The mediastinal pleura is reflected onto the thoracic wall within the costovertebral gutter, and the costal pleura thus extends above the ventral border of the vertebral bodies; the ventral limit of the costal pleura follows an irregular line that passes over the costal cartilages. Cra- nially, the pleural sac extends medially to the first rib and beyond this on the right side where an outpouching (cupula pleurae) passes several centimeters into the neck; this prolongation of the right sac is of potential importance because it may be punctured by penetrating wounds that appear to spare the thorax. The caudal reflection of the costal pleura onto the diaphragm has an unusual line. It begins at the vertebral end of the seventeenth rib and is then deflected caudally to reach the middle of the last rib before turning forward. It then follows a more conventional course that intersects successive ribs at progressively lower levels until it continues along the eighth rib cartilage to the sternum. This line traces a slight dorsocranial concavity (see Figures 20-1 and 20-2Z3).
As always, the pleural cavities are considerably larger than the lungs, even when there is maximal inflation. There thus exist potential spaces along the ventral and caudal margins of the lung that are never utilized. The breadths of these spaces (the costomediastinal and costodiaphragmatic recesses) vary with the phase of respiration. The costodiaphragmatic recess lies over the intrathoracic part of the abdomen and provides a potential route for the puncture of certain abdominal organs. Obviously the risk of injury to the lung is minimized if the needle is introduced during full expiration (see Figure 20-8Z13').