THE LUNGS
The lungs are elongated and shallow, corresponding to the general form of the pleural cavities. The right and left lungs are more nearly equal in size than in other species (Figure 20-5), and because the difference lies mainly in the greater thickness of the right lung, the asymmetry that does exist may easily escape notice (Figure 20-6).
There is no external evidence of lobation other than the presence of the accessory lobe appended to the base of the right lung. However, the cranial part of each lung is somewhat separated from the caudal mass by a relatively attenuated region (see Figures 4-24 and 20-1). The two lungs are extensively joined by connective tissue caudal to the bifurcation of the trachea.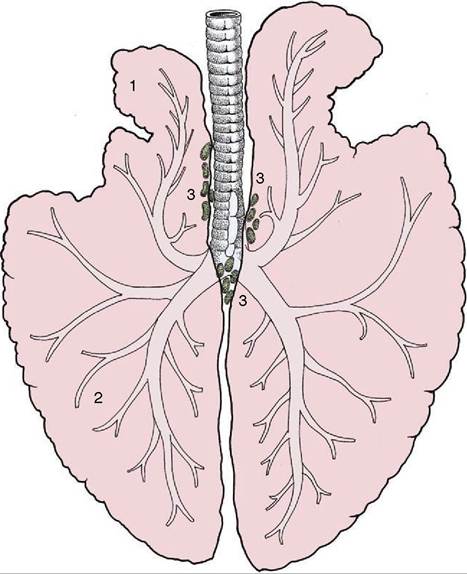
Figure 20-5 Dorsal view of the lungs and bronchial tree, schematic. 1, Apex (cranial lobe) of left lung; 2, base (caudal lobe) of left lung; 3, tracheobronchial lymph nodes.
The left lung exhibits a deep cardiac notch that allows the pericardium extensive contact with the chest wall between the third and sixth ribs (see Figure 20-1). The notch is margined by a thinned region so that the lung provides little cover to the pericardium over a much larger area (Figure 20-7). The arrangement on the right side is similar, although the asymmetry of the heart reduces the size of the cardiac notch, which extends from the third rib to the fourth intercostal space (see Figure 20-2). When moderately expanded, the base of each lung reaches to a line passing through the upper part of the sixteenth, the middle of the eleventh, and the costochondral junction of the sixth rib; the upper part of this line is almost vertical, and the lower part sweeps cranioventrally. This margin of the lung is separated from the line of pleural reflection by about 5 cm dorsally and ventrally but by as much as 15 cm in its middle part (see Figures 20-1 and 20-2).
In young foals the extent of the lung is more restricted and the caudal limit is at about the thirteenth rib.The projection of the lung on the chest wall is considerably larger than the clinically useful area for percussion and auscultation, as examination of the thin margins of the lung will not provide useful information. The area for such examination is triangular and is
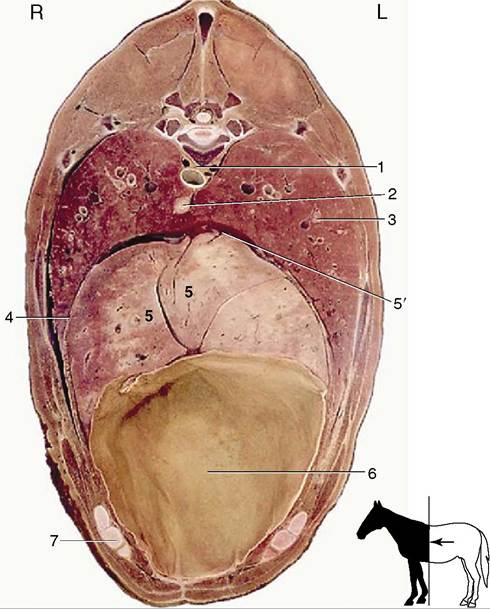
Figure 20-6 Transverse section of the trunk at the level of T12 and the middle of the ninth rib. 1, Aorta; 2, esophagus; 3, lung; 4, diaphragm; 5, liver; 5', caudal vena cava; 6, diaphragmatic flexure of the ascending colon; 7, costal arch.
defined by the caudal angle of the scapula, the point of the elbow, and the upper end of the sixteenth rib. Two sides of this triangle are more or less straight, but the caudoventral side, the hypotenuse, is slightly bowed.
Tapping of pleural fluid is most safely performed in the lower part of the seventh intercostal space, ventral to the margin of the lung. Care is required to avoid puncturing the superficial thoracic (“spur”) vein that crosses the site (see Figure 23-3/11").
The lobulation of the lungs is not obtrusive but can be detected on careful examination of the expanded lung. It is less obvious in the collapsed state when the covering pleura is wrinkled. It is also evident on section. However, it is accepted that the septa are incomplete and that the possibility of collateral ventilation between neighboring lobules exists.
The chief bronchus, the pulmonary artery, and the pulmonary vein combine to form the root of the lung before entering at the hilus in a region deprived of pleura and directly adherent to the same part of the other lung. The chief bronchus separates within the lung into a small cranial division that passes toward
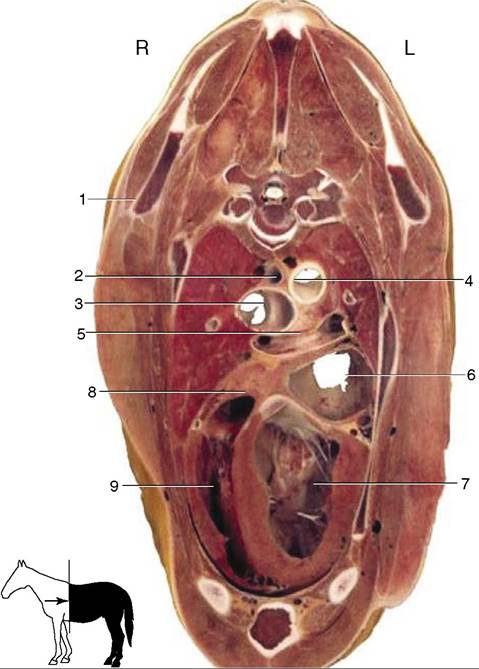
Figure 20-7 Transverse section of the thorax at the level of T5.
1, Caudal angle of scapula; 2, esophagus; 3, bifurcation of the trachea; 4, aorta; 5, bifurcation of the pulmonary trunk; 6, left atrium; 7, left ventricle; 8, right atrium; 9, right ventricle.the cranial lobe and a larger caudal division that attends to the ventilation of the remainder of the organ. There are difficulties in homologizing the bronchi of lower orders with those in other domestic species, but at the present time these details are not of great importance; lung surgery is rarely performed in horses.
In standing animals the ventilation and perfusion of different regions and lobes of the lungs are reasonably well matched, although in larger species, such as the horse, there must be some tendency for gravity to favor the perfusion of more ventral parts. The spatial relationship of ventilation and perfusion is disturbed in animals placed in dorsal or lateral recumbency, and the disturbance becomes significant when the recumbent posture is long maintained—as during major surgery. In these circumstances there is compression of whichever part of the lung is at the bottom. This reduces the tensile forces that ordinarily hold airways open in that part of the lung. The ensuing airway closure permits complete collapse of the alveoli served by such airways; blood perfusing these alveoli cannot take part in respiratory gas exchange.
The pattern of division of the pulmonary artery corresponds to that of the bronchi. A separate bronchial artery attends to the supply of the bronchial and peribronchial tissue, but the blood is returned by the single set of pulmonary veins.
The lymphatic drainage leads first through very small pulmonary nodes embedded in the substance of the organ and then to larger tracheobronchial nodes about the bifurcation of the trachea (Figure 20-3/77). From here most lymph is drained via the cranial mediastinal nodes.
The nerves that enter at the hilus derive from the pulmonary plexus to which both sympathetic and parasympathetic fibers contribute.