» The Shoulder Region and Upper Arm
The scapula and humerus form the bases of the shoulder region and both are wholly included within the skin of the trunk. The slope of the scapula varies considerably and is revealed by the orientation of its spine.
A more sloping shoulder is preferred in saddle horses. The thickened middle portion (tuber spinae) of the spine is readily recognized on palpation and may even provide a visible landmark (Fig. 23.6A/3). The distal part of the spine subsides gradually and does not form an acromion. The bone is extended beyond its dorsal border by a large scapular cartilage that is incorporated within the withers. The margin of the cartilage and the cranial and caudal angles of the bone may be palpated in most subjects. The caudal angle is often quite prominent, even though it is covered by the latissimus dorsi (Fig. 23.3/13).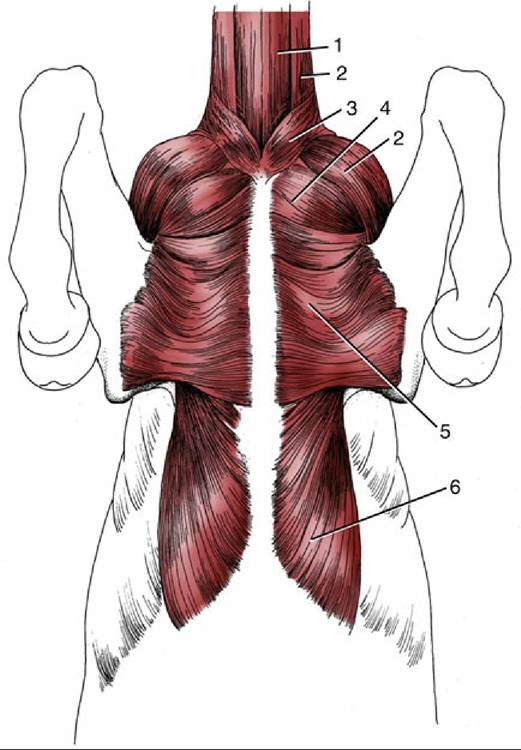
FIG. 23.4 Muscles on the ventral surface of the thorax. 1, Sternocephalicus; 2, brachiocephalicus; 3, cutaneous colli; 4, pectoralis descendens; 5, pectoralis transversus; 6, pectoralis profundus.
The humerus forms a right angle with the scapula and slopes less steeply than in the smaller species. Its surface relief is marked, and many features may be felt through the skin and musculature. The greater and lesser tubercles of the proximal extremity are both well developed and are more nearly equal than those in most species. Each is divided into cranial and caudal parts. The cranial parts are separated by an intertubercular groove that is interrupted by an intermediate tubercle; there are thus five processes. Although both parts of the greater tubercle are easily palpated, its cranial division creates the "point of the shoulder" (Fig. 23.6A/8). Distal to this, the deltoid tuberosity furnishes another easily found landmark (Fig.
23.6A/10).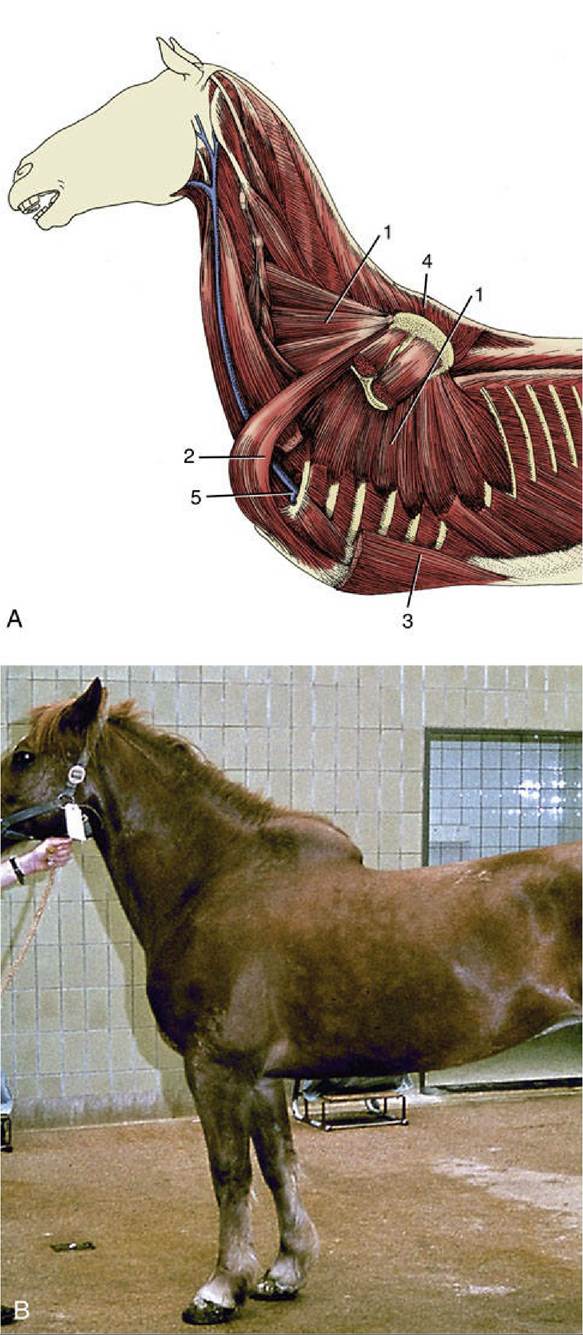
FIG. 23.5 (A) Deep muscles attaching the forelimb to the trunk. 1, Serratus ventralis; 2, subclavius; 3,
pectoralis profundus; 4, rhomboideus; 5, axillary vessels turning around first rib into limb. (B) Rupture of
serratus ventralis muscle.
The shoulder joint has anatomic attributes of a spheroidal joint, but it acts as a hinge joint because of the restrictions imposed by the tendons of the muscles that closely surround the shoulder, notably the infraspinatus (and, to a lesser degree, the supraspinatus) laterally and the subscapularis medially (Fig. 23.7). The relatively capacious joint cavity may be tapped by inserting a needle at the cranial margin of the palpable infraspinatus tendon about 2 cm proximal to the caudal part of the greater tubercle. The needle is directed Ventromedially and must be introduced about 4 or 5 cm before its tip penetrates the capsule. The procedure requires some care because a cranial deflection may cause the needle to enter the bursa that protects the biceps tendon within the intertubercular groove. This intertubercular bursa corresponds to the diverticulum of the joint capsule found in the dog and sheep.
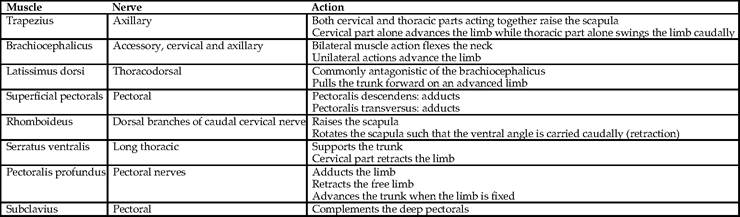
» TABLE 23.1 Girdle Muscles
The muscles that act primarily on the shoulder may be considered as being arranged in lateral and medial groups, although they enclose the joint on all sides. The lateral group comprises the supraspinatus, infraspinatus, deltoideus, and teres minor (Fig. 23.6B).
The supraspinatus (Fig. 23.6B/7) arises from and occupies the supraspinous fossa of the scapula. It bulges beyond the bone cranially where its covering epimysium provides insertion to the subclavius. It splits into two short tendons that straddle the origin of the biceps before attaching to the cranial parts of the tubercles of the humerus.
The muscle is placed to extend the shoulder joint, but its most important function may be stabilization of the joint.The infraspinatus (Fig. 23.6B/8) is located in the infraspinous fossa, and its insertion crosses the lateral aspect of the shoulder joint before separating into deep and superficial tendons. The short deep tendon attaches to the edge of the caudal part of the greater tubercle. The superficial tendon crosses this projection to attach at a more distal level and is protected by a synovial bursa where it lies against the bone. Inflammation of the bursa may be painful and may cause the animal to stand with the affected limb abducted at the shoulder, which is a posture that relieves the pressure at the site. The infraspinatus is primarily a shoulder fixator whose tendon substitutes for a lateral collateral ligament. It has a secondary abductor action. Both the supraspinatus and the infraspinatus are supplied by the suprascapular nerve.
The deltoideus (Fig. 23.6B/9) arises from the caudal border and spine of the scapula; the latter origin is indirect and effected by way of an aponeurosis that covers the infraspinatus. The insertion is to the deltoid tuberosity, which is used as a landmark to trace the muscle proximally. It is partly recessed within a depression of the triceps, and the line between the muscles is sometimes visible in thin-skinned animals. The deltoideus is a shoulder flexor with a secondary role as abductor of the arm. Innervation is by the axillary nerve.
The unimportant teres minor is buried by the deltoideus over the caudolateral aspect of the shoulder joint.
The medial muscle group comprises the subscapularis, teres major, coracobrachialis, and capsularis, of which the last is of trivial significance. The subscapularis arises from and occupies the subscapular fossa (Fig. 23.8/1). It inserts on the lesser tubercle and, though primarily employed to stabilize the joint, may also function as an adductor of the arm. It is supplied by the subscapular nerve.
The teres major (Fig. 23.8/3) arises from the caudal angle of the scapula. It is contained between the subscapularis and the latissimus dorsi and inserts in common with the latter. It is chiefly a flexor of the shoulder but may also adduct the arm. It is supplied by the axillary nerve, as are all the true flexors of the shoulder.
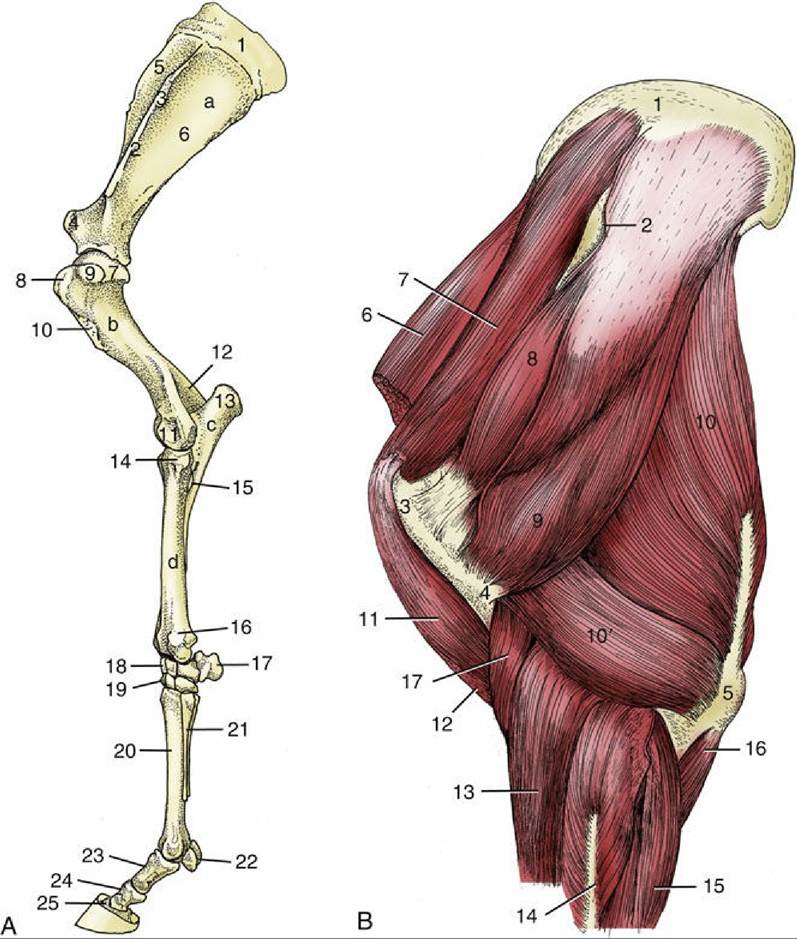
FIG. 23.6 (A) Skeleton of the left forelimb, lateral view. a, Scapula; b, humerus; c, ulna; d, radius; 1, scapular cartilage; 2, scapular spine; 3, tuberosity of scapular spine; 4, supraglenoid tubercle; 5 and 6, supraspinous and infraspinous fossae, respectively; 7, head of humerus; 8 and 9, cranial and caudal parts of greater tubercle, respectively; 10, deltoid tuberosity; 11, condyle; 12, olecranon fossa; 13, olecranon;
14, tubercle for lateral collateral ligament; 15, interosseous space; 16, lateral styloid process; 17, accessory carpal; 18 and 19, proximal and distal row of carpal bones, respectively; 20, large metacarpal (cannon) bone; 21, small metacarpal (splint) bone; 22, proximal sesamoid bones; 23, proximal phalanx;
24, middle phalanx; 25, distal phalanx. (B) Muscles associated with shoulder and elbow joints, lateral view. 1, Scapular cartilage; 2, scapular spine; 3, greater tubercle of humerus; 4, deltoid tuberosity of humerus; 5, olecranon; 6, subclavius; 7, supraspinatus; 8, infraspinatus; 9, deltoideus; 10, long head of triceps; 10', lateral head of triceps; 11, biceps; 12, lacertus fibrosus; 13, extensor carpi radialis; 14, common digital extensor; 15, ulnaris lateralis; 16, ulnar head of deep digital flexor; 17, brachialis.
The coracobrachialis (Fig. 23.8/8) arises from the coracoid process on the medial aspect of the supraglenoid tubercle and inserts on the proximal part of the shaft of the humerus. It is an adductor of the arm but is of little consequence. It is supplied by the musculocutaneous nerve (Table 23.2).