» The Shoulder Region and Upper Arm (see also pp. 6870 and 73-75)
The scapula and humerus form the basis of the shoulder and upper arm, including the shoulder joint. Whereas the acromion on the distal end of the scapular spine and the greater tubercle are easily recognized on visual inspection, the following anatomic features may be located on palpation: the full length of the spine; the cranial border, angle, and dorsal border of the scapula; the tendon of origin of the biceps; the deltoid tuberosity; and the medial and lateral surfaces of the shaft of the humerus (these are revealed by grasping the bone between the fingers of one hand).
The attachment of the pectoral muscles to cranial parts of the bones near the shoulder joint prevents palpation of the medial surface of both the joint and the upper part of the humerus.The superficial cervical lymph nodes cranial to the scapula are most easily palpated with the limb retracted (see Fig. 2.55/4), whereas the axillary lymph nodes, located on the thoracic wall caudal to the shoulder joint, can be palpated with the limb protracted—but only when they are enlarged. Both these groups drain the forelimb. An accessory axillary lymph node draining local skin and muscles and the thoracic mammary glands is inconstantly present on the thoracic wall dorsal to the olecranon (see Fig. 2.55/10).
The scapula is covered laterally by the trapezius, supraspinatus, and infraspinatus (Fig. 16.1), with the tendons of the latter two muscles crossing the joint to attach to the humerus. The belly of the infraspinatus is suitable for intramuscular injections. The flexor aspect of the joint is covered by the deltoideus, which connects the scapular spine with the deltoid tuberosity (Table 16.2).
The shaft of the humerus is overlain laterally by the long head of the triceps, cranially by the biceps (itself partly covered by the brachiocephalicus), and on different aspects by the brachialis as it winds around the bone and by other heads of the triceps.
In contrast, the medial surface, once free of the pectoral muscles, is relatively uncovered, which allows the brachial vessels and the nerve trunks heading for the distal portion of the limb to lie close to the bone (Fig. 16.2).In craniocaudal radiographs of the extended shoulder joint, the supraglenoid tubercle overlaps the head of the humerus; in lateral radiographs this tubercle is superimposed on the greater tubercle of the humerus (Fig. 16.3A, C, and C'/2). In dogs younger than 3 to 5 months the supraglenoid tubercle is still separated from the rest of the scapula by cartilage. The proximal epiphysis for the tubercles and head of the humerus commonly fuses with the shaft at about 10 months (but several months later in larger breeds). In the cat the coracoid process, on the medial aspect of the supraglenoid tubercle, is a pronounced cylindric swelling with a separate ossification center. The flat coracobrachial muscle originates from the coracoid process and passes over the subscapularis insertion tendon, from which it is separated by a bursa, before running caudodistally over the medial aspect of the shoulder joint to end on the proximal part of the humerus. It adducts the arm and rotates the shoulder joint outward. The feline acromion is broadened by a flat, caudally directed (suprahamate) process (see Fig. 2.45D), which overhangs the infraspinatus muscle slightly. In the cat, an extra ossification center is also present for the lesser tubercle. The clavicle of the dog is represented by a small ossicle cranioventral to the shoulder joint. In the cat the vestigial clavicle takes the form of a slender rodlet, roughly 2 cm long, in the corresponding location; it is regularly depicted in radiographic films and may be palpated against the cranial aspect of the joint (Fig. 16.3C '/5).
In both cats and dogs, the capsule of the shoulder joint extends a diverticulum that invests the biceps tendon of origin, including the part that is secured in the intertubercular groove of the humerus by a transverse ligament extending between the greater and lesser tubercles.
The lack of collateral ligaments on the spheroidal shoulder joint is partly compensated by the minor local thickenings of the capsule (glenohumeral ligaments) in addition to the transverse ligament already mentioned. The swellings of the shoulder joints are difficult to detect because of the overlying muscles.» TABLE 16.1
Development and Maturation of the Forelimb Skeleton
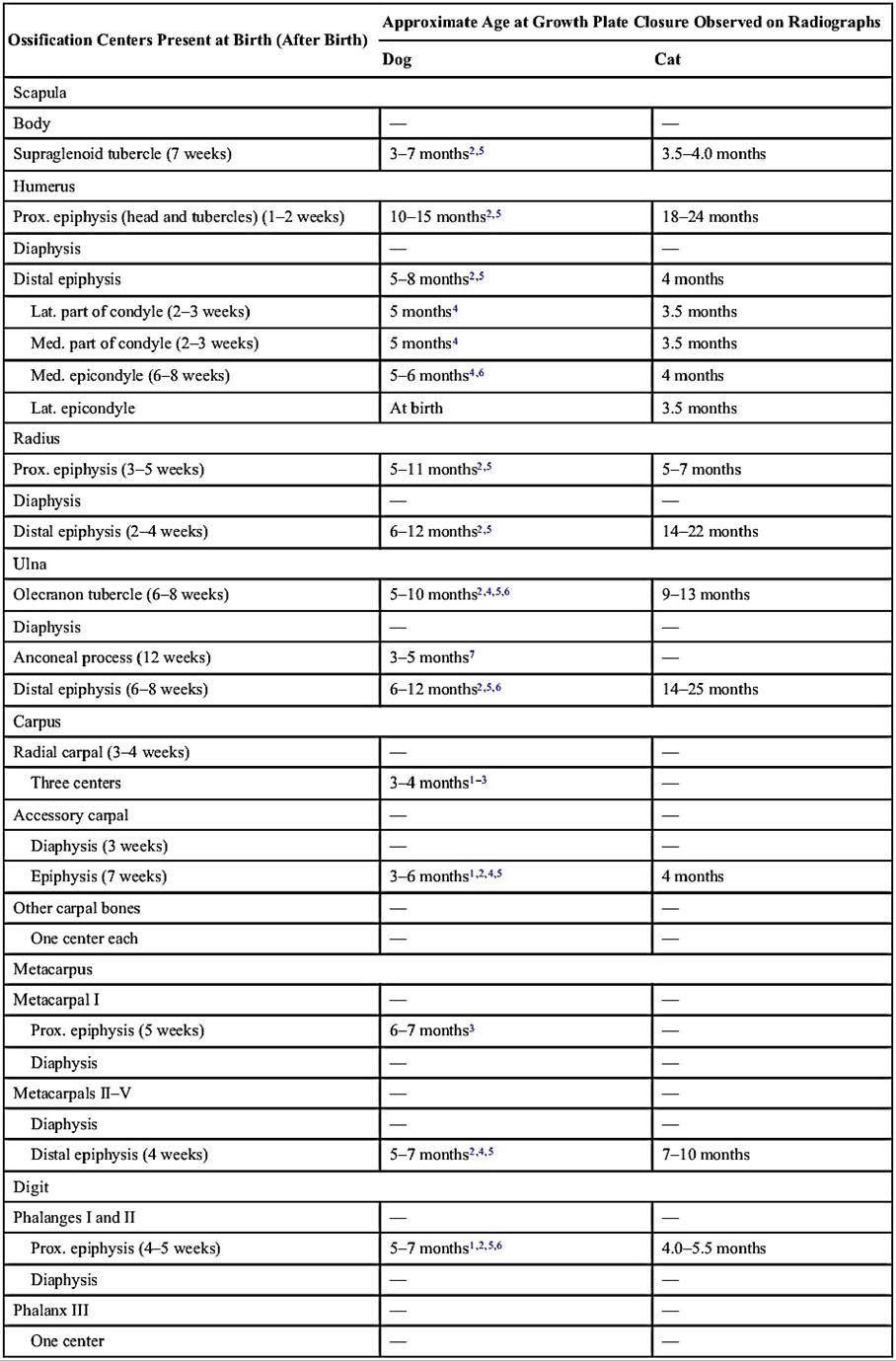
Lat., Lateral; Med., medial; Prox., proximal.
1 Based on Chapman WL: Appearance of ossification centers and epiphyseal closures as determined by radiographic techniques, JAVMA 147:138-141,1965.
2 Based on Hare WCD: The age at which epiphyseal union takes place in the limb bones of the dog, Wien Tierarztl Monatsschr 9:224-245, 1972.
3 Based on Pomriaskynski-Kobozieff N, Kobozieff N: Etude radiologique de l’aspect du squelette normal de la main du chien aux divers Stades de son evolution de la naissance a l’age adult, Rec Med Vet 130:617-646, 1954.
4 Based on Smith RN, Allcock J: Epiphyseal fusion in the Greyhound, Vet Rec 72:75-79, 1960.
5 Based on Sumner-Smith G: Observations on the epiphyseal fusion of the canine appendicular skeleton, J Small Anim Pract 7:303-311, 1966.
6 Based on Ticer JW: Radiographic technique in small animal practice, Philadelphia, 1975, Saunders, p. 101.
7 Based on Van Sickle D: The relationship of ossification to elbow dysplasia, Anim Hosp 2:24-31,1966.
From de Lahunta A and Habel RE: Applied veterinary anatomy, Philadelphia, 1986, Saunders.
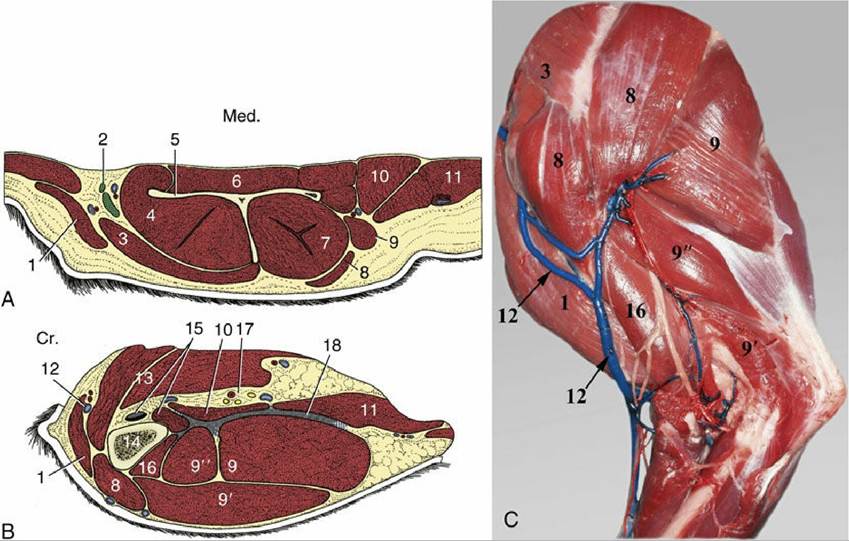
FIG. 16.1 Transverse sections of the left canine forelimb at the level of the scapula (A) and just distal to the shoulder joint (B) and lateral view (C). 1, Brachiocephalicus; 2, superficial cervical lymph nodes; 3, omotransversarius; 4, supraspinatus; 5, scapula; 6, subscapularis; 7, infraspinatus; 8, deltoideus; 9, 9', and 9", long, lateral, and accessory heads of triceps, respectively; 10, teres major; 11, latissimus dorsi; 12, cephalic vein; 13, pectoral muscles; 14, humerus; 15, biceps tendon and coracobrachialis; 16, brachialis;
17, brachial vessels and nerve trunks; 18, heavy intermuscular fascia.
Cr., Cranial; Med., medial.The luxations of the shoulder joint occur when structures that support the joint are broken as a result of trauma. Most of the luxations occur medially or laterally. The rupture of the transverse ligament that restrains the biceps tendon in the bicipital groove lets the tendon slip over the lesser tubercle when the shoulder is flexed. This is a painful condition with the shoulder joint in a permanently extended state.
It is useful to remember, for purposes of orientation, that the distal end of the acromion is opposite the joint space. The glenoid concavity is considerably smaller than the head of the humerus, which considerably increases the range of movement. The relative looseness of the joint permits abduction of the humerus in sedated or anesthetized dogs and cats; it is then possible to puncture the capsule midway between the acromion and the greater tubercle by passing a needle mediocaudally through the deltoideus.
The teres minor muscle, deep to the deltoid muscle on the flexor aspect of the shoulder, runs between the distal part of the caudal margin of the scapula and the teres minor tuberosity. In the cat teres minor is covered by the infraspinous and triceps muscles and becomes stronger and more effective by fusing with the tendon of the latissimus dorsi. The flat tensor fasciae antebrachii muscle located over the medial surface of the triceps muscle arises by means of a broad aponeurosis from the latissimus dorsi and radiates into the forearm fascia. It acts as a tensor of the fascia and an extensor of the elbow joint. The triceps muscle has already been described (p. 77).
Luxation of the joint and fractures of the scapula are both relatively rare. Because the clavicle lacks a functional connection with the trunk, the entire joint appears to "ride with the blow" when subjected to a sudden external force. Fractures of the humerus are much more common and mostly occur at midshaft level. Malignant tumors of the proximal humerus and the distal radial metaphyses are relatively more common in the large and the so-called giant breeds of dog compared to small dogs and cats.
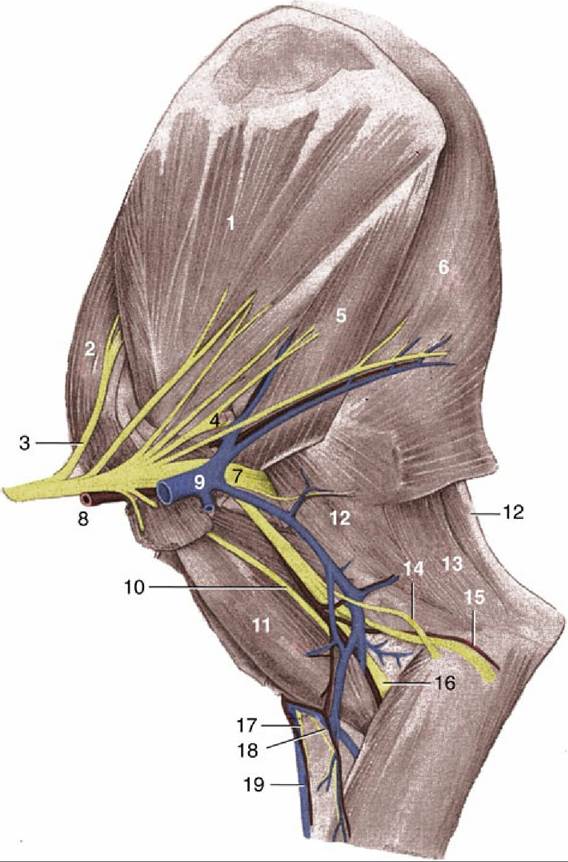
FIG. 16.2 Medial surface of the right canine shoulder and arm. 1, Subscapularis; 2, supraspinatus; 3, suprascapular nerve; 4, axillary nerve; 5, teres major; 6, latissimus dorsi; 7, radial nerve; 8, axillary artery;
9, axillary vein; 10, musculocutaneous nerve; 11, biceps; 12, long head of triceps; 13, tensor fasciae antebrachii; 14, caudal cutaneous antebrachial nerve; 15, ulnar nerve and collateral ulnar artery; 16, median nerve and brachial artery; 17, medial branch of superficial radial nerve; 18, median cubital vein;
19, cephalic vein.