» The Elbow and Forearm (see also pp. 70-71, 74, and 7880)
Both the medial and lateral aspects of the elbow joint are conveniently accessible because the arm is relatively free and the axillary fossa is deep. The most prominent feature of the region, the summit of the olecranon, is located just below the ventral end of the fifth intercostal space in a dog standing square.
The medial and lateral epicondyles and adjacent parts of the humerus are all easily palpated. The bundle composed of the brachial vessels and median nerve can be palpated against the medial surface of the bone, between the biceps and triceps. The smaller bundle formed by the collateral ulnar vessels and ulnar nerve may be located against the triceps tendon and olecranon (see Fig. 16.13/5 and 6). The collateral ligaments arising from the epicondyles are also easily palpated. Although the condyle of the humerus projects forward and is offset from the long axis of the bone, a considerable covering of muscle makes it less accessible.The entire medial border of the radius is subcutaneous. However, the cranial surface is palpable distally, where it is only thinly covered by the extensor carpi obliquus and the tendons of the other extensors (Fig. 16.4/6). The ulna is more deeply placed except at its distal end, where its styloid process connects with the carpal bones. A deep depression behind this process is bounded by the prominent tendon of the flexor carpi ulnaris and the accessory carpal bone.
The median vessels (Fig. 16.4/3) (continuations of the brachial) and nerve are embedded among the carpal and digital flexor muscles, close to the medial border of the radius (Fig. 16.5).
Arteries: Axillary → Brachial → Median → Radial
Veins: Cephalic; Median → Brachial → Axillary
The cephalic vein (Fig. 16.4/1), the most popular choice for intravenous injections, follows the cranial border of the forearm, where it can be palpated when raised by pressure over the elbow; it often produces a visible ridge even when not occluded in this way.
Because it is connected (by the median cubital vein) to the deep system of veins at the elbow before it continues over the lateral surface of the arm, it is best compressed distal to this anastomosis (Fig. 16.6/2). The vein lies on the extensor carpi radialis in the forearm, accompanied by sensory branches of the radial nerve.In cats, the distal end of the humerus is distinguished by a prominent medial (supracondylar) foramen (Figs. 2.46C/14 and 16.7), which transmits the brachial artery and median nerve in the caudocranial direction. These structures are therefore vulnerable in fractures and surgery of this part.
Lateral radiographs show the humeral condyle deeply seated in the trochlear notch of the ulna (Fig. 16.8A). The prominent medial epicondyle (Fig. 16.8/1') is superimposed on the olecranon, while the anconeal process, at the proximal end of the notch (Fig. 16.8/4), is superimposed in turn on the medial epicondyle. In some breeds the anconeal process may have its own ossification center that fuses with the rest of the bone at 3 to 5 months of age. If it fails to do so (un-united anconeal process or elbow dysplasia), as occurs in fast growing large breed dogs, or if, having fused, it later becomes detached, the loose piece causes severe lameness. The medial coronoid process at the distal end of the trochlear notch (Fig. 16.8/5) is not formed from a separate ossification center, and its separation is therefore not due to a developmental failure but to another cause, such as osteochondrosis or fracture resulting from overloading. The medial coronoid process is superimposed on the proximal end of the radius in lateral radiographs of the normal joint.

FIG. 16.3 Lateral (A, C and C') and craniocaudal (B and D) radiographic views of the canine (A and B) and feline (C, C', and D) shoulder joints; C and D were taken from specimens. 1, Scapular spine; 1,, acromion; 2, supraglenoid tubercle; 3, greater tubercle of humerus; 4, head of humerus; 5, vestigial clavicle.
The distal epiphysis of the humerus fuses with the shaft at 5 to 8 months, which is considerably earlier than closure at the proximal end. The proximal epiphyseal cartilage of the radius and that of the tuber olecrani generally disappear about the same time; the larger distal cartilages of the forearm bones disappear a little later, usually at about 6 to 9 months. Fully two-thirds of the lengthening of the radius is due to growth at its distal cartilage. The lengthening of the ulna (distal to the elbow joint) is almost equally dependent on growth of its V-shaped distal cartilage. The deformation that follows unequal elongation of these bones results from "premature fusion" of one of the distal growth cartilages; the most prominent effect is deviation of the paw, which tenses several interosseous connective tissue structures, most notably the distal part of the radioulnar ligament. Differences in growth velocity between the radius and ulna may also be responsible for incongruity at the elbow joint, which causes a step to develop between the normally level articular surfaces of the radius and ulna.
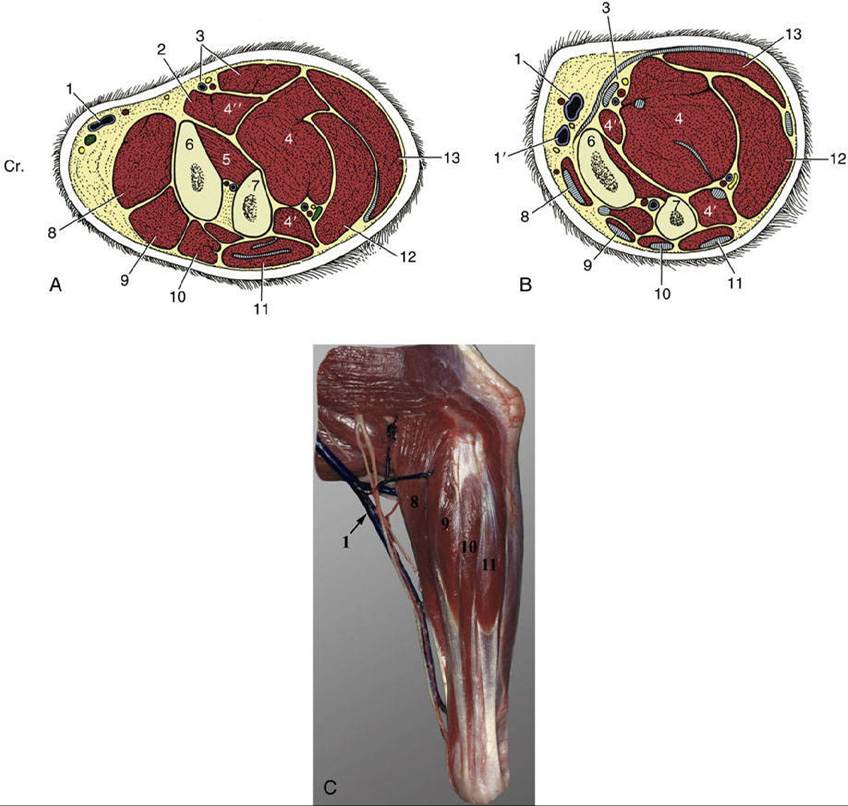
FIG. 16.4 Transverse sections of the left canine forelimb just distal to the elbow joint (A) and just proximal to the carpus (B) and lateral view (C). 1, Cephalic vein and branches of superficial radial nerve; 1', accessory cephalic vein; 2, pronator teres; 3, median vessels and nerve and flexor carpi radialis; 4, 4', and 4", humeral, ulnar, and radial heads of deep digital flexor, respectively; 5, pronator quadratus; 6, radius; 7, ulna; 8, extensor carpi radialis; 9, common digital extensor; 10, lateral digital extensor; 11, ulnaris lateralis; 12, flexor carpi ulnaris—its small ulnar head lies on its caudal aspect, and the ulnar vessels and nerve lie on its cranial aspect; 13, superficial digital flexor; Cr., cranial.
In the dog, the distal part of the humerus presents three ossification centers: that for the capitulum, the trochlea, and the medial epicondyle.
The latter is reported to be liable to separate in young dogs of the larger breeds, which causes relocation of the origin of the flexor carpi radialis muscle. In the cat an additional ossification center is found in the lateral epicondyle.Forearm fractures are relatively common. They occur most often in the distal half of the forearm and, as would be anticipated, generally involve both bones. Fracture of the olecranon is also fairly common.
Flexion of the elbow is accomplished by the brachialis and biceps brachii. The brachial muscle originates from the caudal part of the proximal humerus and winds over the lateral surface to gain the medial aspect of the elbow before inserting on the radial and ulnar tuberosities. The biarticular biceps arises from the supraglenoid tubercle and in the dog divides its insertion between the medial coronoid process of the ulna and the radial tuberosity. A tendon strap of no obvious functional significance is sometimes present between the biceps and the extensor carpi radialis muscle. The biceps of the cat inserts only on the radial tuberosity. This muscle has some supinator capacity. The extensor group comprises the triceps, tensor, and anconeus (to be mentioned shortly).
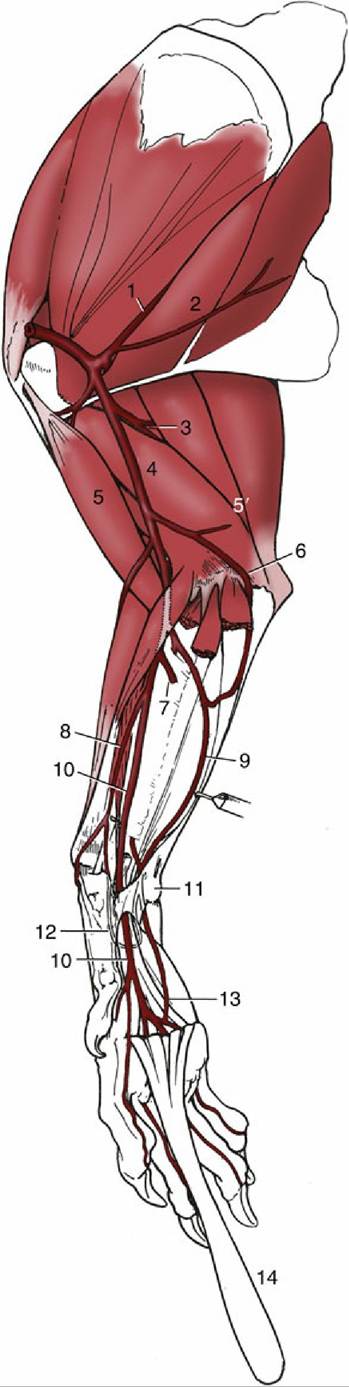
FIG. 16.5 The topography of the major arteries of the right canine forelimb, medial view. The caudomedial muscles of the forearm have been removed. 1, Subscapular artery; 2, teres major; 3, deep brachial artery; 4, brachial artery; 5, biceps; 5', triceps; 6, collateral ulnar artery; 7, deep antebrachial artery; 8, radial artery; 9, ulnar artery; 10, median artery; 11, accessory carpal bone; l2, deep palmar arch; 13, superficial palmar arch; 14, superficial digital flexor, reflected.
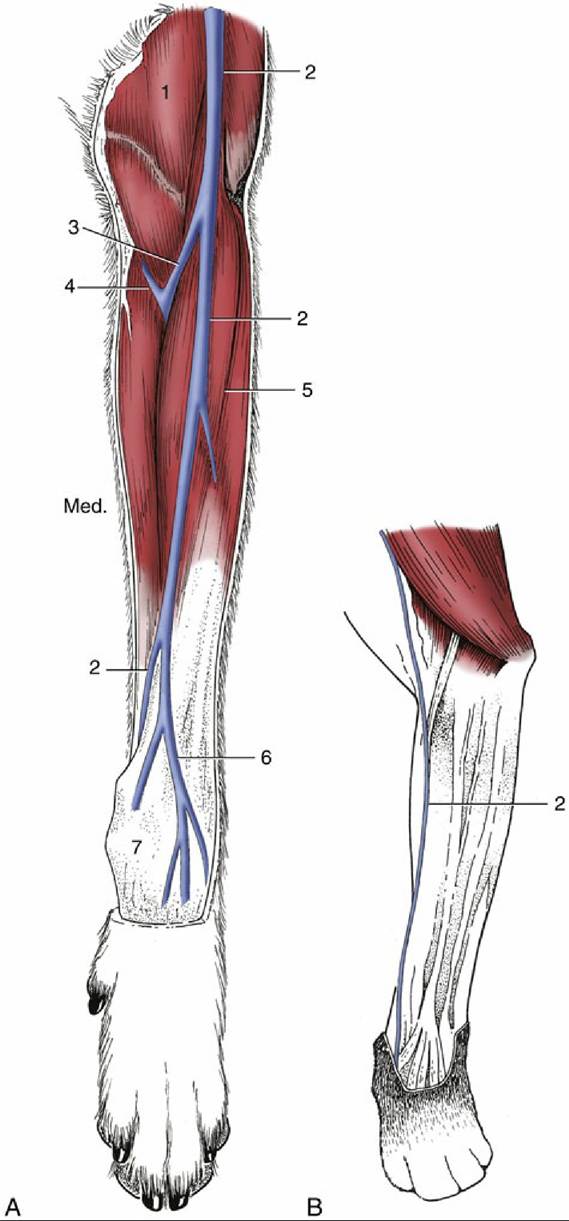
FIG. 16.6 (A) Superficial veins on the left canine forearm. (B) The course of the cephalic vein on the left feline forearm.
1, Brachiocephalicus; 2, cephalic vein; 3, median cubital vein; 4, brachial vein; 5, extensor carpi radialis; 6, accessory cephalic vein; 7, carpus; Med., medial.FIG. 16.7

Feline humerus exhibiting the supracondylar foramen (1).
The movements of supination, in which the dorsal surface of the paw is turned outward, and pronation, in which it is turned inward, are primarily the task of a small group of dedicated muscles: two supinators and two pronators. The essential movement is of course rotation of the radius within the embrace of the ulna. The supinator is a small, flat, fusiform muscle that lies deep to the extensor muscles in the forearm. It originates from the lateral epicondyle of the humerus and adjacent structures and inserts on the dorsal surface of the proximal quarter of the shaft of the radius, reaching close to the medial border of this bone. The second supinator, the brachioradialis, is very weak or even absent in the dog and constant but hardly important in the cat, in which it forms a thin ribbon running close to the cephalic vein. The pronator teres comes from the medial epicondyle of the humerus and converges on the supinator; the two muscles insert close together. The pronator teres is stronger in the cat than in the dog. The pronator quadratus lies medial to the interosseous membrane that joins the radius and ulna along the length of their shafts, and, like this membrane, it runs between the two bones.
The elbow joint capsule, common to the joint between the humerus and the radius and ulna and to the proximal joint between the forearm bones, extends three pouches: craniolaterally beneath the common digital extensor, craniomedially beneath the biceps, and caudally between the lateral epicondyle and the olecranon. The last is used for injections in cats, whereas the first site is more often preferred in dogs. The caudal part of the capsule is closely related to the small, flat anconeus muscle, usually assigned to the extensors of the elbow but probably more important as a tensor of the capsule, preventing redundant folds of synovial membrane from being nipped between the bones.
Luxation of the elbow joint is relatively common. The joint is most easily luxated through lateral displacement of the radius and ulna when it is flexed because the anconeal process withdraws from the olecranon fossa of the humerus. Lateral luxation may also occur following trauma, which may rupture or avulse the collateral ligaments. Medial luxation is less frequent, probably because it is more difficult for the anconeal process to snap over the larger medial epicondyle. It follows that dislocations will be most easily reduced if the joint is first strongly flexed to disengage the anconeal process.
In both dogs and cats the collateral ligaments of the elbow present both radial and ulnar divisions, and there are differences in the relative strength of the parts in the two species. The differences influence the relative degrees of pronation and supination. The cat actively enjoys 100 degrees or more of movement, whereas the passive excursions in the dog are limited to about 50 degrees of supination and 20 degrees of pronation. The annular ligament that completes the ring within which the head of the radius rotates inserts on the cranial part of the medial coronoid process, which is consequently subjected to considerable tensile stress. A small sesamoid bone is occasionally associated with the lateral collateral ligament.
The muscles of the forearm conform in broad outline to the common pattern previously described (pp. 78-80), and any differences in their arrangements are not of functional significance. The extensors of the carpus and digit, lying cranial to the shaft of the radius, are separated from the flexors caudal to the bone by the palpable border of the radius medially and by the attachment of the most lateral extensor, the ulnaris lateralis, to the salient and easily identified accessory carpal bone laterally. Apart from acting as an abductor of the carpus, the ulnaris lateralis appears to support extension of an already extended carpal joint or flexion of one already flexed. The existence of a bridge (interflexorius) crossing from the deep to the superficial digital flexor muscle in the distal forearm may be mentioned as a distinctive feature of carnivores, among the domestic species.

FIG. 16.8 Lateral (A) and craniocaudal (B) radiographic views of the elbow joint of a young dog (A and B) and of a cat (C, C', and D). The (feline) supracondylar foramen is depicted in Fig. 16.7. 1, Humerus; 1', medial epicondyle; 1", supratrochlear foramen; 2, radius; 2', proximal epiphyseal cartilage; 3, ulna; 3', olecranon; 3", apophysis of tuber olecrani; 4, anconeal process; 5, medial coronoid process; Med., medial.