THE SKELETON OF THE LEG AND HOCK; THE HOCK JOINT
The tibia is the only functional component of the skeleton of the leg. Its shaft is thickly covered by muscle on its craniolateral and caudal aspects but is subcutaneous medially (Figure 24-7/7).
The distal articular surface, known as the cochlea, comprises two grooves separated by a ridge, all with a craniolateral inclination. The cochlea is flanked by medial and lateral malleoli (Figure 24-8/2,2').The fibula is much reduced. The proximal extremity or head forms a tight articulation with the lateral condyle of the tibia (Figure 24-1/9). The head usually continues into a short and rodlike shaft, but sometimes a band of soft tissue intervenes; this may simulate a fracture when depicted in a radiograph. In later embryonic life the isolated distal extremity of the fibula becomes assimilated within the tibia to which it furnishes the lateral malleolus (see Figure 2-59, D,E/6'). The independence of the malleolar center of ossification is clearly evident in radiographs of young animals, and the line of union may be evident in the adult bone.
The hock (Figure 24-8) comprises the following elements: talus and calcaneus in the proximal row, a central tarsal bone in the intermediate row, and fused first and
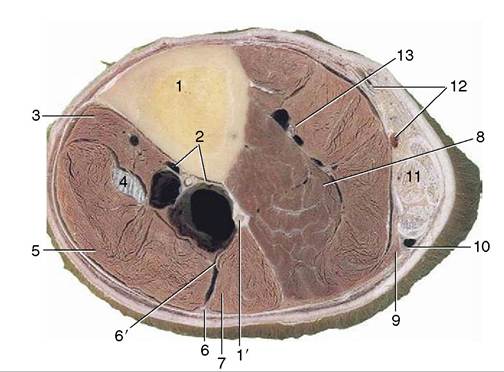
Figure 24-7 Transverse section of the left leg slightly above its middle. 1, Tibia; 1', fibula; 2, cranial tibial vessels; 3, tibialis cranialis; 4, peroneus tertius; 5, long digital extensor; 6, 6', superficial and deep peroneal nerves; 7, lateral digital extensor; 8, deep digital flexors; 9, soleus; 10, lateral saphenous vein and caudal cutaneous sural nerve; 11, superficial digital flexor surrounded by the other components of the common calcanean tendon (gastrocnemius and tarsal tendons of semitendinosus and biceps); 12, caudal branch of medial saphenous vein, tibial nerve, and saphenous artery; 13, caudal tibial vessels.
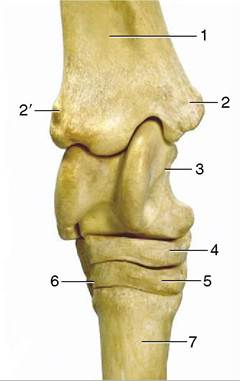
Figure 24-8 Dorsal view of the right hock. 1, Tibia; 2, medial malleolus; 2', lateral malleolus; 3, talus with trochlea; 4, central tarsal bone; 5, third tarsal bone; 6, fourth tarsal bone; 7, third metatarsal (cannon) bone.
second bones and separate third and fourth bones in the distal row. The proximodorsal surface of the talus (Figure 24—8/5) carries an oblique trochlea corresponding to the cochlea of the tibia. The distal surface is more or less flat and rests on the central bone. The calcaneus (Figure 24-9/4,4') lies largely to the plantar aspect of the talus; the tuber surmounting the calcanean process rises about 5 cm above the tarsocrural joint space and serves as a rough guide to that feature. The composite bone formed by the first and second tarsal bones is relatively small and lies mainly behind the much larger, wedge-shaped third tarsal (Figure 24-8/5). The fourth bone (Figure 24-8/6) on the lateral side) is cuboidal, unlike the other bones in the distal row, which are flattened; its greater depth causes it to occupy both the intermediate and the distal tiers. The bones of the distal row articulate with the metatarsal bones, that is, the third (cannon) bone centrally and the much smaller second and fourth (splint) bones to the sides.
Even cursory examination of the tarsal skeleton is sufficient to make it plain that while free movement is allowed at the tarsocrural joint, there can be almost no play at any other level. The obliquity of the articular surfaces of the tibia and talus ensures that the distal part of the limb is carried outward as well as forward when the hock joint is flexed.
The fibrous layer of the joint capsule extends from the tibia to the metatarsus. It is firmly attached over various parts of the skeleton but is free elsewhere and then varies considerably in strength; the weaker parts (pouches) bulge when the synovial sac is distended.
Numerous ligaments are associated with the hock, but the majority are short and are conveniently regarded as mere local thickenings of the capsule. Three that are larger and more discrete are of greater importance. Paired collateral ligaments extend from the malleoli to the corresponding splint bones and may be palpated along their whole lengths (see Figure 24-10, D/9,9'). They have intermediate attachments to the bones they cross, and these help ensure that movements of the hock are restricted to flexion and extension at the tarsocrural level. A long plantar ligament (Figure 24-10, D/10) follows the plantar aspect of the calcaneus, passes over the fourth tarsal, and then continues distally onto the proximal part of the metatarsus. It is largely covered by the tendon of the superficial digital flexor but may be palpated to each side of this. It is commonly strained about the middle of its length, and in lateral view the resulting thickening gives a convex profile to the plantar aspect of the hock. The condition is known as a curb (from the French courbe, curve, contour).The hock is a compound joint with three joint sacs: one common to the tarsocrural and proximal intertarsal levels, one for the distal intertarsal level, and one for the tarsometatarsal level (Figure 24-9/10-15). The two more distal sacs are small and occasionally communicate; the distal intertarsal sac may be punctured from the medial side, while access to the tarsometatarsal sac may be gained between the fourth tarsal and the head of the splint bone. The novice will find neither technique very reliable. The proximal part of the talocrural sac is capacious and is prone to overdistention, which causes the capsule to pouch at its weakest points. There are three such pouches. One, at the dorsomedial aspect of the hock, is bounded by the tendon of the peroneus tertius, the medial collateral ligament, the medial malleolus, and the medial branch of the tendon of the tibialis cranialis (Figure 24-10, D/8 and Figure 24-10, A-C).
The sac is easily punctured here, even when it is not distended; care must be taken to avoid the cranial branch of the medial saphenous vein, which crosses the site. The second and third pouches are on the plantar aspect. One is found between the medial collateral ligament and the deep flexor tendon at the level of the medial malleolus; the other is behind the lateral collateral ligament, between the calcaneus and the lateral malleolus. Unless the joint sac is considerably distended, puncture at either of these sites may prove difficult.Swelling of the joint sac may be confused with swelling of the synovial (tarsal) sheath around the deep flexor tendon (Figure 24-10/5"). The differential diagnosis is simple. When the joint sac is distended, pressure applied to either plantar pouch is transmitted to the dorsal pouch (and vice versa). Swelling of the tarsal sheath is transmitted from plantaromedial to plantarolateral (or vice versa) if local pressure is applied; it is
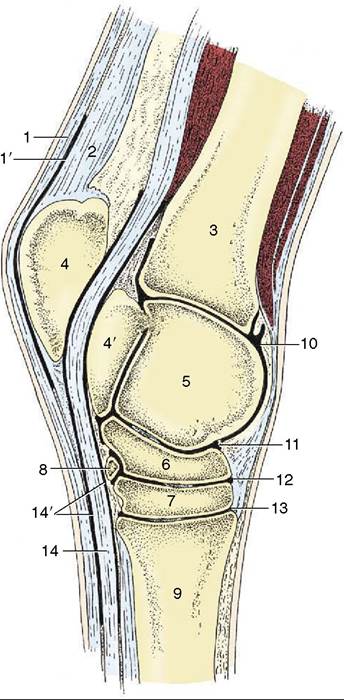
Figure 24-9 Sagittal section of the hock joint. 1, Superficial digital flexor; 1', subtendinous calcanean bursa; 2, gastrocnemius; 3, tibia; 4, calcaneus; 4', sustentaculum tali; 5, talus; 6, central tarsal; 7, third tarsal; 8, fourth tarsal (mainly on lateral side); 9, large metatarsal (cannon) bone; 10, tarsocrural joint; 11, proximal intertarsal joint (communicates with 10); 12, distal intertarsal joint; 13, tarsometatarsal joint; 14, deep digital flexor; 14', tarsal sheath.
not transmitted to the dorsal aspect of the joint. Moreover, the swelling of the tendon sheath is evident about 5 cm proximal to the plantar swelling of the joint.
Arthritic changes (spavin) commonly affect the bones of the hock. The changes most commonly begin on the medial aspect, near the meeting of the third and central tarsal and third metatarsal bones. This region, the “seat of spavin,” is crossed by the medial branch of the tibialis cranialis tendon (the cunean tendon of clinical authors) (Figure 24-10/7) en route to its insertion on the combined first and second tarsal bones. The tendon is a useful reference point because it is palpable. A portion is sometimes resected for the purposes of reducing pressure over the lesion and eliminating movement between the distal tarsal elements. The treatment is often effective in reducing pain, although obviously it does not cure the condition.