The Skeletonand Carpal Joint
The shaft of the radius is flattened from front to back and is covered by muscle on all but its subcutaneous medial border. The distal extremity broadens to meet the expanded carpus (commonly known as the "knee").
On each side it carries a styloid process and, proximal to this, an eminence for the attachment of a collateral ligament. The cranial aspect is grooved for the passage of the extensor tendons. These tendons, the adjacent molding of the bone, the styloid processes, and the eminences for ligamentous attachment are all very distinctly palpable.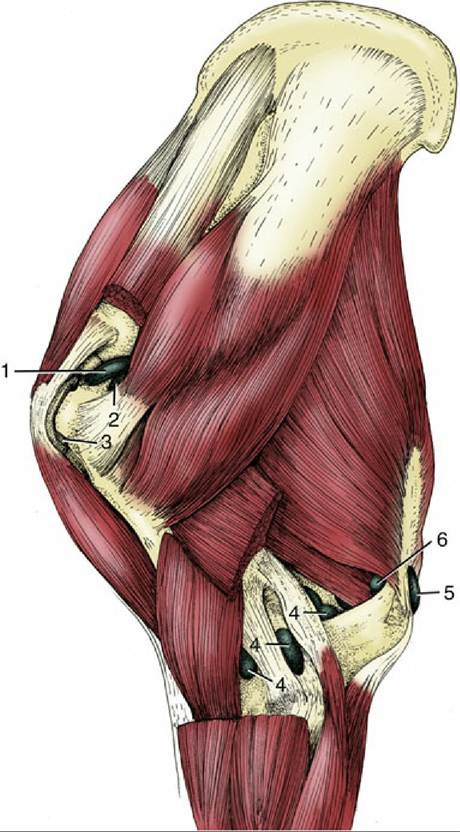
FIG. 23.11 Synovial structures of the left shoulder and elbow regions, lateral view. 1, Shoulder joint capsule; 2, infraspinatus bursa; 3, intertubercular bursa (between biceps tendon and humerus); 4, elbow joint capsule; 5, subcutaneous olecranon bursa; 6, subtendinous olecranon bursa. (For identification of the muscles, see Fig. 23.6B.)
The carpal skeleton is arranged in the usual two rows (see Fig. 23.20A). The proximal row comprises radial, intermediate, and ulnar carpal bones, concerned in weight-bearing, together with a laterally flattened, discoidal accessory bone that projects backward in a very conspicuous fashion. The accessory bone articulates with the lateral styloid process and the ulnar carpal but bears no weight. The distal row is also deep; in addition to three constant elements — second, third, and fourth carpal bones—there is often a pea-shaped first carpal. This bone is frequently isolated from the remainder of the skeleton, embedded in the palmar carpal ligament behind the second carpal; it may be mistaken for a bone fragment when shown in radiographs (Fig. 23.13/6).
Fractures of the carpal bones are mostly caused by repetitive loading and jumping. For example, the "slab fracture" commonly occurs in the frontal plane of the third carpal bone.
Thoroughbred horses experience accessory carpal bone fracture during jumps over fences or collisions. Collision accidents or kicks may also cause multifragment fractures.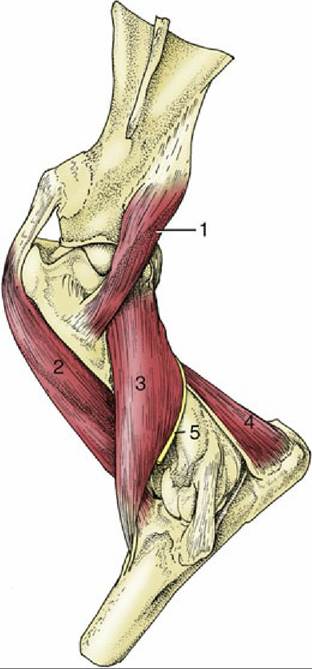
FIG. 23.12 Deep muscles of the left shoulder and elbow joints, lateral view. 1, Teres minor; 2, biceps; 3, brachialis; 4, anconeus; 5, radial nerve.
The carpal joint is maintained in full extension in the standing posture but is capable of very considerable flexion. It presents three levels of articulation. Movement is most free at the radiocarpal (antebrachiocarpal) level, where as much as 90 or 100 degrees of flexion is allowed. The midcarpal articulation is also mobile, allowing perhaps 45 degrees of flexion, but no significant movement is possible at the carpometacarpal level (Fig. 23.13B). The articular surfaces of the bones reflect these differences (Fig. 23.14A). The radial articular surface shows some demarcations corresponding to the three proximal carpal bones but overall presents a caudal hemicylindrical ridge and narrow cranial gutter. The upper surfaces of the proximal carpal bone row have the reciprocal conformation. Their lower surfaces are convex in front and concave behind. The surfaces at the distal joint are broadly flat. Fig. 23.15A illustrates these features and the two axes of rotation. The fronts of the bones are driven together in full extension of the joint and may splinter ("chip fractures"*) during the fast gaits.
The carpus is mainly supported by the cannon bone but also makes contact with the bases of the splint bones. Indeed, so large a part of the second carpal bone rests on the second metacarpal that it may tend to drive that bone away from the cannon bone, leading to painful acute inflammation known as "splints." This condition is more common at the medial intermetacarpal joint.
» TABLE 23.3
Arm Muscles: Flexors
| Muscle | Nerve | Action |
| Biceps brachii | Musculocutaneous | Fixes and extends the shoulder May also flex the elbow Tendon stores and releases energy for rapid gait |
| Brachialis | Musculocutaneous and some contribution from radial | Flexes the elbow |
» TABLE 23.4
Arm Muscles: Extensors

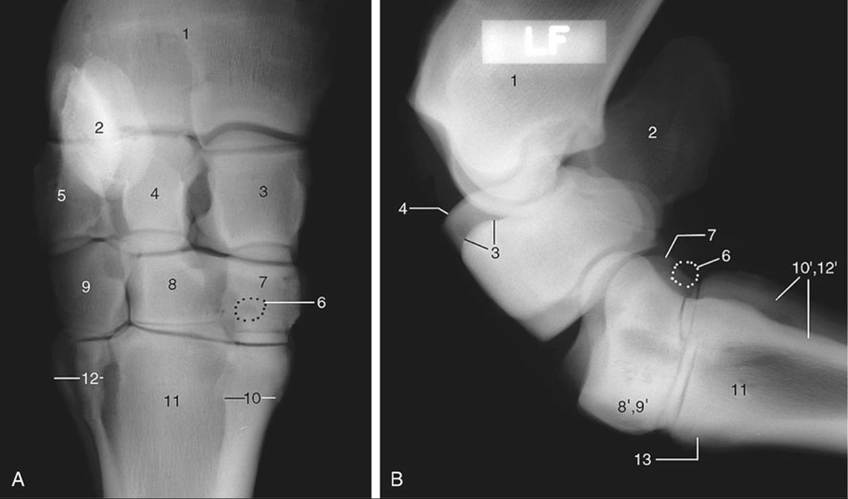
FIG.
23.13 (A) Dorsopalmar and (B) lateral radiographs of the carpus. 1, Radius; 2, accessory carpal (faint); 3, radial carpal; 4, intermediate carpal; 5, ulnar carpal; 6, position of first carpal, when present; 7, 8, and 9, second, third, and fourth carpals, respectively; 8' and 9', superimposed third and fourth carpals, respectively; 10, 11, and 12, second, third, and fourth metacarpals, respectively; 10' and 12', superimposed second and fourth metacarpals, respectively; 13, metacarpal tuberosity.The three levels of articulation share a common fibrous capsule, but the synovial compartments are separate except for a narrow communication between the middle and distal levels (Fig. 23.14). The fibrous capsule (Fig. 23.15A/3), which has extensive connections with all the bones involved in the joint, is of very unequal thickness. It is weakest dorsally, where it is rather loose in the extended position of the joint. It is much thicker over the palmar aspect (Fig. 23.15/7), where it opposes overextension. This part, the palmar carpal ligament, fills the irregularities of the bones and smooths the backward-facing aspect of the carpal skeleton. Medial and lateral collateral ligaments extend between the lower end of the radius and the upper part of the metacarpus. They have intermediate attachments to the carpal bones to restrict the joint movement to the sagittal plane. There are numerous additional ligaments that collectively stabilize the joint through joining of adjacent bones in the same row or distal bones to the metacarpus. Others secure the accessory bone, including one that runs obliquely from its distal edge to the metacarpus and forms a conspicuous ridge. A larger transverse ligament (flexor retinaculum; Fig. 23.15B/22) extends from the palmar edge of the accessory bone to attach at the mediopalmar aspect of the joint. It completes the enclosure of a space, the carpal canal, through which pass the flexor tendons and other structures en route from the forearm to the distal part of the limb.
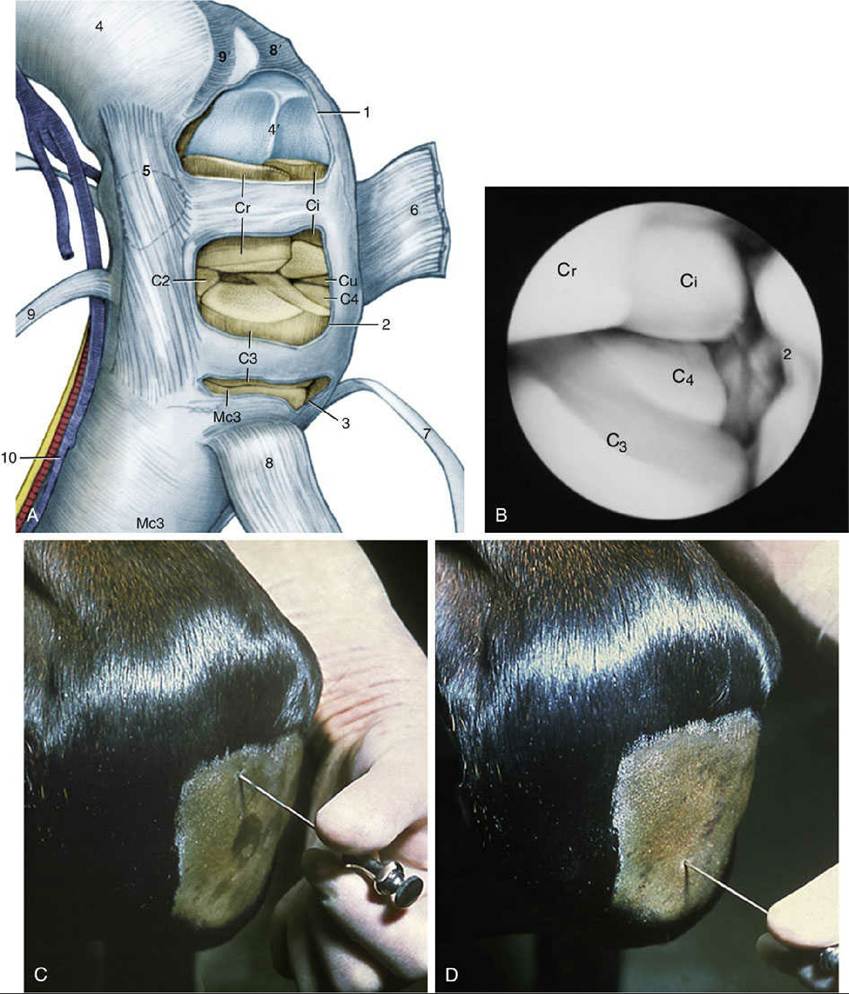
FIG. 23.14 (A) Flexed left carpus, dorsomedial view. The articular surfaces are stippled. (B) Arthroscopic medial-to-lateral view of the left midcarpal joint. Cr, Ci, and Cu, Radial, intermediate, and ulnar carpal bones, respectively; C2, C3, and C4, second, third, and fourth carpal bones, respectively; Mc3, third metacarpal (cannon) bone. 1, Radiocarpal joint capsule, fenestrated; 2, midcarpal joint capsule, fenestrated in A; 3, carpometacarpal joint capsule, fenestrated; 4 and 4', radius and its distal articular surface, respectively; 5, position of bursa between medial collateral ligament and extensor carpi obliquus (9); 6, extensor retinaculum, reflected; 7, common digital extensor; 8 and 8', extensor carpi radialis and its groove on radius, respectively; 9 and 9', extensor carpi obliquus and its groove on radius, respectively; 10, medial palmar nerve, artery, and vein. (C) Puncture of radiocarpal joint. (D) Puncture of midcarpal joint.
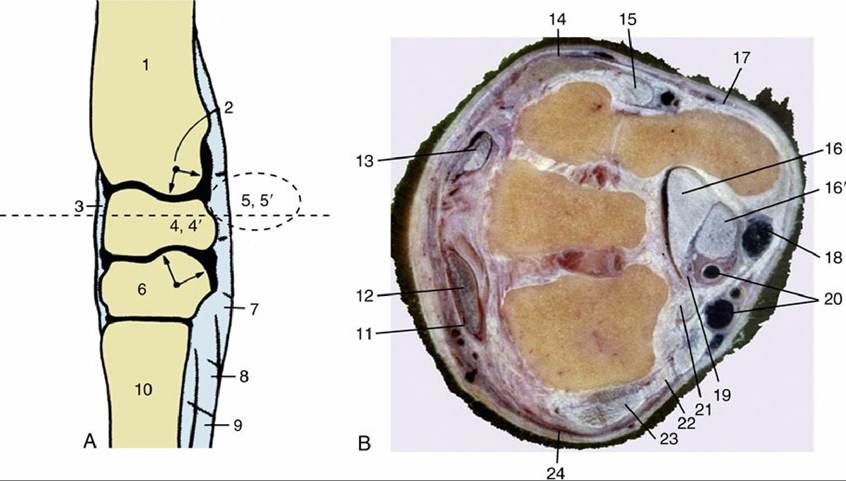
FIG. 23.15 (A) Axial section of the carpus. The broken transverse line indicates level of section in B. 1, Radius; 2, axis of rotation; 3, fibrous joint capsule; 4 and 4', intermediate and radial carpal, respectively; 5 and 5', accessory and ulnar carpal, respectively; 6, third carpal; 7, palmar carpal ligament; 8, accessory (check) ligament of deep digital flexor; 9, interosseus; 10, large metacarpal. (B) Transverse section of the right carpus, proximal surface. Both joints face to the left. 11, Extensor retinaculum; 12, extensor carpi radialis; 13, common digital extensor; 14, lateral digital extensor; 15, long tendon of ulnaris lateralis; 16 and 16', deep and superficial flexor tendons in carpal canal, respectively; 17, dorsal branch of ulnar nerve; 18, palmar branch of median artery and lateral palmar nerve; 19, median artery and medial palmar nerve;
20, radial artery and vein; 21, flexor carpi radialis; 22, flexor retinaculum; 23, medial collateral ligament;
24, extensor carpi obliquus.
Distention of the radiocarpal joint capsule is not uncommon (Fig. 23.16/1). The capsule pouches where support is weak, dorsally between the extensor tendons and proximally above the accessory bone, just caudal to the lateral digital extensor tendon. It may be punctured here, but a more convenient approach is from the dorsal aspect. Flexion of the carpus opens up the joint space, facilitating the entry of a needle between the extensor tendons. A similar approach may be made to the middle compartment (Fig. 23.14C and D).