The Tendons, Annular Ligaments, and Interosseus Muscle
The tendons of the common and lateral digital extensors enter the foot to the front of the metacarpal bone; those of the superficial and deep flexors enter behind it. A third very important element in the support of the fetlock, the tendinous interosseus muscle, is situated on the palmar aspect, between the bone and the flexor tendons.
The structures on the palmar surface of the cannon are enclosed within a deep fascia that extends from one splint bone to the other. The fascia is thickest immediately below the carpus but gradually thins when followed distally, and toward the fetlock it offers little hindrance to the palpation of deeper structures.The common digital extensor tendon is protected by a synovial bursa as it passes over the dorsal pouch of the fetlock joint. Broadening, it makes limited attachments at the proximal borders of PI and PII before receiving the extensor branches of the interosseus that wind around the digit. It ends on the extensor process of PIII (Figs. 23.27/1 and 23.26/17).
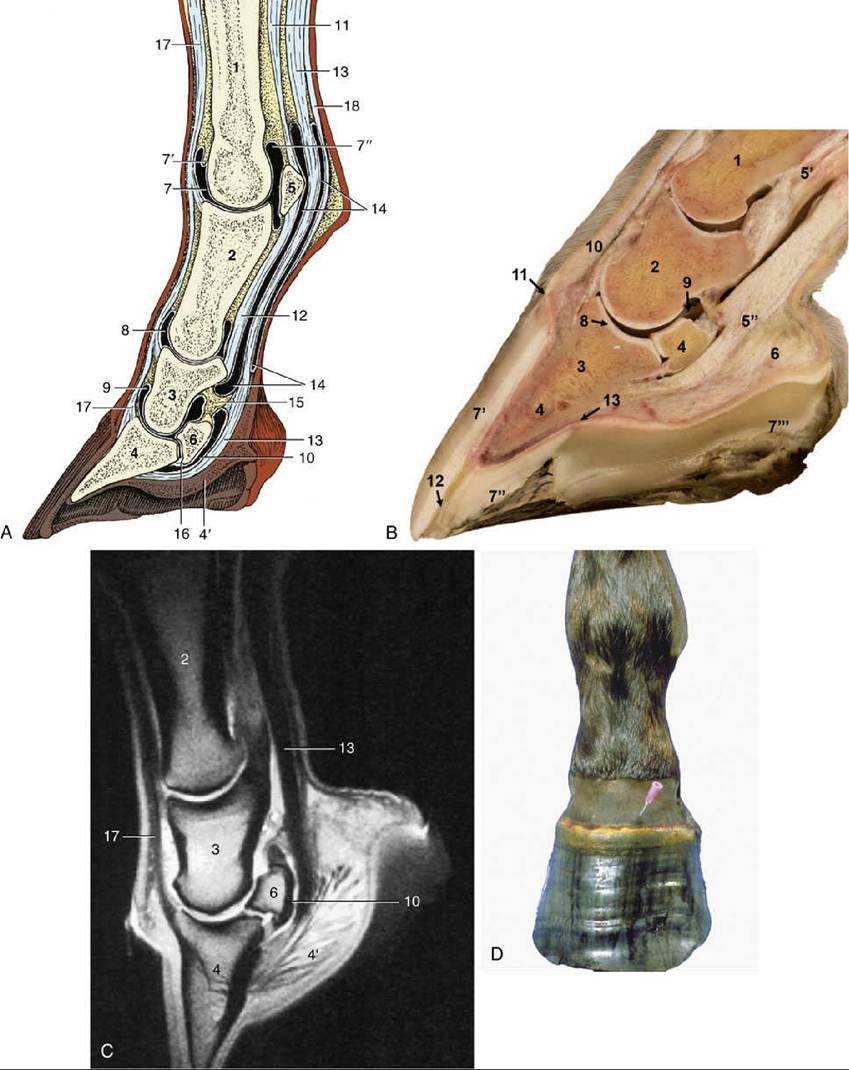
FIG. 23.26 (A) Axial section of digit (semi-schematic). (B) Axial section of digit with latex-injected fetlock, pastern, and coffin joints. (C) Corresponding magnetic resonance image. (D) Puncture of coffin joint. 1, Large metacarpal bone; 2, proximal phalanx; 3, middle phalanx; 4, distal phalanx; 4', digital cushion; 5, proximal sesamoid bone; 6, distal sesamoid (navicular) bone; 7, dorsal pouch of fetlock joint; 7', capsular fold; 7", palmar pouch of fetlock joint; 8 and 9, dorsal pouches of pastern and coffin joints, respectively; 10, navicular bursa; 11, interosseus; 12, straight sesamoidean ligament; 13, deep flexor tendon; 14, digital sheath; 15, connective tissue bridge; 16, distal navicular ligament; 17, common digital extensor tendon;
18, superficial flexor tendon.
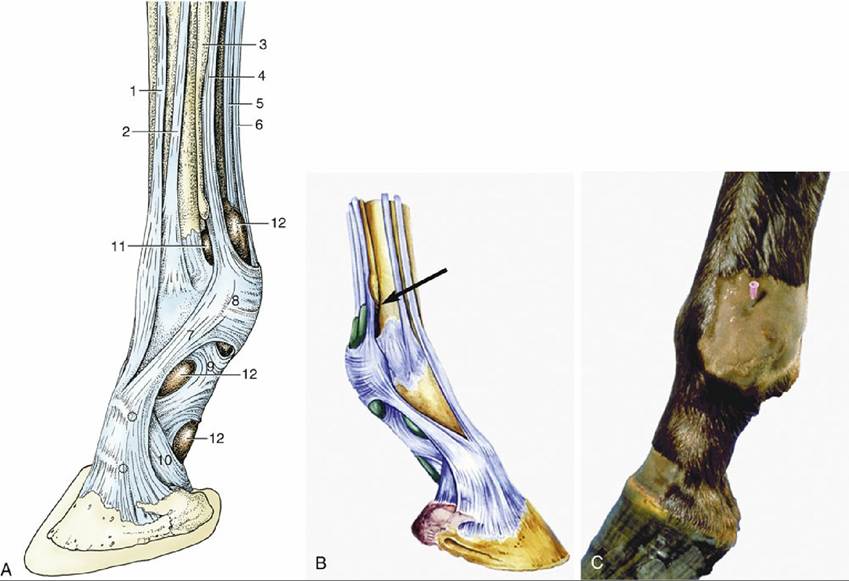
FIG. 23.27 (A) Tendons and annular ligaments of the left digit, dorsolateral view. The two dotted circles indicate the sites for injecting the pastern and coffin joints. 1, Common digital extensor; 2, lateral digital extensor; 3, lateral splint bone; 4, interosseus; 5, deep digital flexor; 6, superficial digital flexor; 7, extensor branch of interosseus; 8, palmar annular ligament; 9, proximal digital annular ligament; 10, distal digital annular ligament; 11, palmar pouch of fetlock joint; 12, digital sheath. (B) Schematic drawing of right digit showing digital sheath (green) and palmar pouch of fetlock joint (arrow). (C) Puncture of fetlock joint.
The lateral digital extensor tendon descends on the metacarpal bone lateral to the common tendon, crosses the fetlock joint, and ends on a roughening on the dorsal aspect of PI. Both extensor tendons, though easily palpated in the metacarpus, evade recognition beyond the fetlock joint, where they become broader and thinner. The extensor branches of the interosseus are more prominent below the skin.
The superficial digital flexor tendon becomes subcutaneous (except for the fascial investment of distally decreasing thickness) after emerging from the carpal canal and provides the caudal border of the cannon. It forms a sleeve around the deep flexor tendon at the level of the proximal sesamoid bones (Fig. 23.28B). The deep part of the sleeve splits opposite the middle of PI to allow the superficial flexor to attach to the distal tubercles of PI and the adjacent complementary fibrocartilage of PII. The palmar part of the sleeve ends at about the same level to allow the deep flexor tendon to gain the superficial position, where it is palpable for a few centimeters before it enters the hoof.
Only the medial and lateral borders of the deep digital flexor tendon can be palpated above the fetlock. The tendon is most easily separated and distinguished from that of the superficial flexor muscle when the fetlock joint is flexed to relieve tension, but even in these circumstances, it is usually impossible to identify the very strong accessory (check) ligament that arises from the palmar carpal ligament to join the deep face of the tendon toward the middle of the cannon (Fig.
23.18/14'). The tendon then passes the fetlock in the sleeve formed by the superficial tendon, and beyond the middle of PI it rides over the bearing surface provided by the complementary fibrocartilage of PII. It then widens before passing over the navicular bone to terminate on PIII.Lameness: Recent data obtained with magnetic resonance imaging and computed tomography have shown that inflammation of the deep digital flexor tendon is the most common soft tissue injury that leads to lameness in the horse.
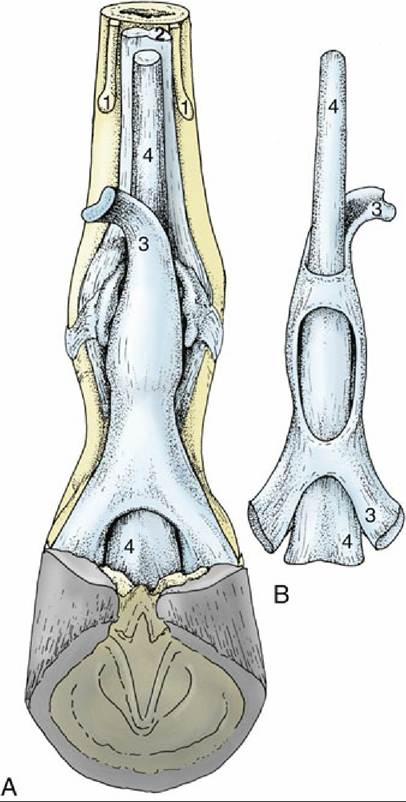
FIG. 23.28 Relations and topography of the superficial and deep flexor tendons. (A) Palmar view, in situ.
(B) Dorsal view, isolated. 1, Splint bones; 2, interosseus; 3, superficial digital flexor; 4, deep digital flexor.
The flexor tendons are held in place by three annular ligaments, which are local thickenings of the deep fascia. The first, the palmar annular ligament, arises from the abaxial borders of the proximal sesamoid bones. Because the ligament adheres to the superficial flexor tendon, the potential for movement between the tendon and the sesamoids is clearly restricted. The second, the proximal digital annular ligament, resembles an X when viewed from behind (Fig. 23.29/6). The proximal margin of the X and the four corners, which attach near the proximal and distal tubercles of PI, are most easily distinguished because the body and the distal margin fuse with the superficial tendon. The third, the distal digital annular ligament, arises from the medial and lateral borders of PI together with the abaxial palmar ligaments of the pastern joint. It provides a sling that fuses with the palmar surface of the deep tendon, continuing to the insertion on PIII within the hoof, and separates the tendon from the digital cushion. Usually, only its free upper border can be demonstrated (Fig. 23.29/7).
The repetitive excessive strain or external trauma may cause pathology of flexor tendons.
The navicular (podotrochlear) bursa protects the deep flexor tendon from excessive friction and pressure against the navicular bone (Fig. 23.26/10). Nonseptic inflammation of the navicular bursa or its adhesions with the deep digital flexor tendon can occur in navicular disease. More proximally, the tendon shares a complex synovial (digital) sheath (Fig. 23.26/14) with the superficial flexor tendon. The sheath begins a few centimeters proximal to the fetlock joint and ends level with the middle of PII (Fig. 23.26B). It lubricates the passage of the tendons over the bearing surfaces and under the free parts of the annular ligaments and facilitates their movements against each other where they exchange position. It is a common site of inflammation and, when distended, bulges most noticeably above the proximal sesamoid bones. Although the sheath is in close proximity to the fetlock, pastern, and coffin joints and to the navicular bursa, these cavities do not communicate, except for a connection between the sheath and the coffin joint in the foal. Despite this, anesthetics injected into the coffin joint of adult horses reach the navicular bursa by diffusion.The interosseus muscle is a strong, flat, predominantly tendinous band, better known as the suspensory ligament. The small contingent of muscle fibers in the interosseous plays an important role in dampening the concussion and consequent heat generation in this tendinous structure. The interosseus arises from the palmar carpal ligament and adjacent part of the large metacarpal bone, descends between the splint bones, and divides a short distance above the fetlock. The two divisions are substantial—and easily palpable—and insert on the abaxial surface of the proximal sesamoid bones. Each detaches a weak (extensor) branch that winds around PI to join the common extensor tendon at the level of the pastern joint (Figs. 23.23/1 and 23.27/7).
A functional continuation of the interosseus beyond the sesamoid bones is provided by the cruciate, oblique, and straight sesamoidean ligaments as described earlier (Fig. 23.23/4 and 5). These support the normally overextended fetlock joint, and the sesamoids permit frictionless movement over the flexor aspect of the joint (Fig. 23.26/5, 11, and 12). Energy, stored within the apparatus (and in the flexor tendons) by stretching on hoof impact, is released at the end of the stride, which allows the joint to flex and impart forward impetus.