THE URINARY BLADDER
The bladder is a distensible storage organ and thus can have no constant size, position, or relationships. It is small and globular when fully contracted and is then
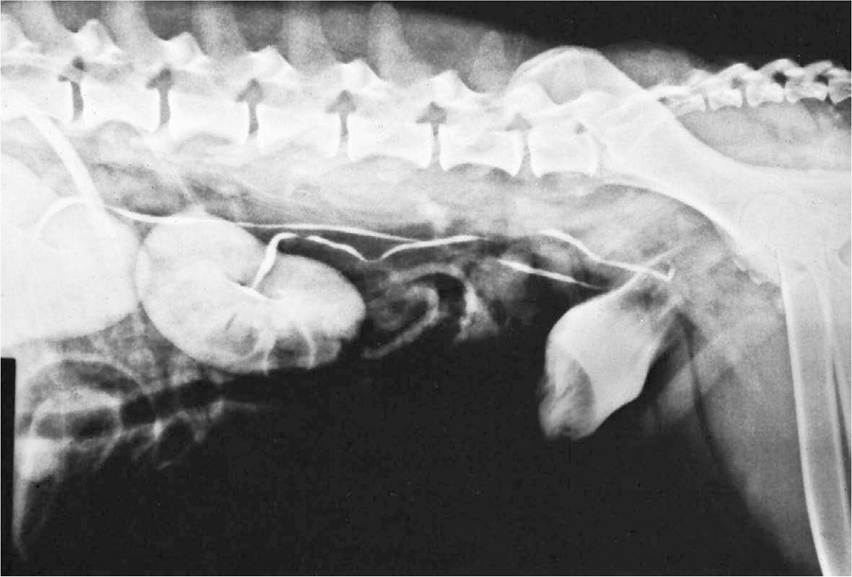
Figure 5-30 Radiograph of renal pelves, ureters, and bladder of the dog.
remarkable for the great thickness of its walls and the negligible extent of its lumen. The contracted bladder rests on the pubic bones; it is confined to the pelvic cavity in the larger species but extends into the abdomen in carnivores. When the bladder enlarges it becomes pear-shaped, presenting a cranial vertex (apex), an intermediate body, and a caudal neck that narrows to the internal urethral orifice at the junction with the urethra. Although continuing distention carries an everincreasing portion of the bladder into the abdomen, the neck remains fixed within the pelvis through its continuity with the urethra (Figure 5-32/11).
No immediate increase in internal pressure occurs when the bladder begins to fill. However, once a certain, quite considerable volume has been attained, the pressure rises sharply; this creates the urge to void urine, an urge that is obeyed without hesitation in many species. In house-trained animals the urge may temporarily disappear if resisted, although discomfort and, later, pain may be experienced if the bladder becomes overfull. In the well-trained dog the distention may be very great, carrying the apex cranial to the umbilicus and stretching the walls to paper thinness with risk of rupture. Though the outline of the grossly distended bladder is smooth, that of the more modestly distended organ is irregular as the low internal pressure allows it to be indented by its firmer neighbors (see Figure 5-30).
In the larger species the contracted bladder is largely retroperitoneal, but most of the surface becomes intraperitoneal when the organ is even moderately expanded.
Three folds continue this serosal covering onto the abdominal and pelvic walls (Figure 5-33). Paired lateral vesical folds convey the round ligaments of the bladder; these vestiges of the umbilical arteries retain narrow lumina through which some blood reaches the cranial part of the bladder. The third, median vesical fold, is empty in the adult, but in the fetus it supports the urachus, the constricted cranial continuation of the bladder that passes forward to leave the abdomen through the umbilical foramen before expanding externally into the allantoic sac. Urachus and umbilical arteries rupture at birth; the urachus survives as a scar on the bladder vertex, while the umbilical arteries are transformed into the round ligaments. The folds in the adult bound the ventral pair of the several excavations into which the pelvic peritoneal cavity is divided (see Figures 22-6 and 22-7).The constant dorsal relations of the bladder are to the reproductive organs and their supporting folds: the uterus and vagina within the broad ligament in the female and the deferent duct (and perhaps the vesicular glands) within the genital fold in the male. The bladder may also make indirect contact with the rectum through these folds. The ventral surface touches the pelvic and
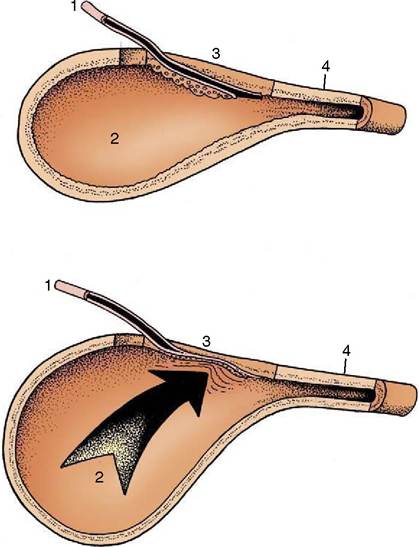
Figure 5-31 The ureterovesical junction. Because of its oblique passage through the wall, the ureter is compressed as the intravesical pressure rises. 1, Ureter; 2, bladder lumen; 3, bladder wall; 4, bladder neck.
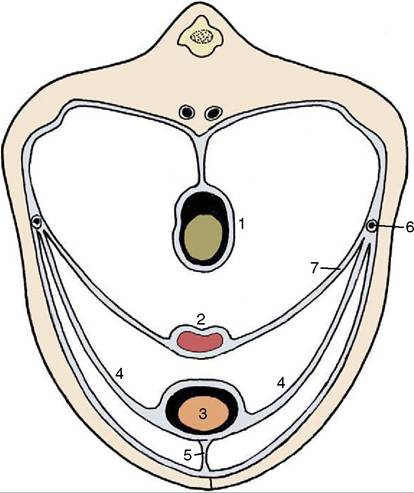
Figure 5-33 Peritoneal disposition in the caudal part of the abdomen. 1, Colon; 2, uterus; 3, bladder; 4, lateral vesical ligaments; 5, median vesical ligament; 6, ureter; 7, broad ligament of uterus (mesometrium).
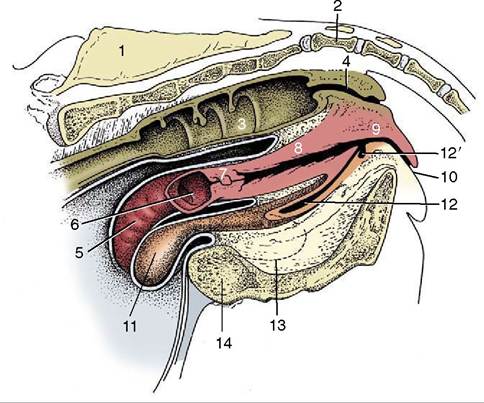
Figure 5-32 Median section of the bovine pelvis.
1, Sacrum; 2, first caudal vertebra; 3, interior of rectum; 4, anal canal; 5, exterior of right uterine horn; 6, interior of stump of left uterine horn; 7, cervix; 8, vagina; 9, vestibule; 10, vulva; 11, exterior of bladder; 12, urethra; 12’, suburethral diverticulum; 13, obturator foramen; 14, pelvis symphysis.abdominal floor. Other relations of the intraabdominal part of the bladder are less predictable and may be numerous when the bladder is greatly enlarged.
The loose attachment of the bladder mucosa and its ability to stretch allow marked change in the appearance of the interior with altered physiological status. The surface, much folded when the lumen is small, becomes generally smooth when the bladder fills. However, two particular folds resist effacement. These run from the slitlike orifices of the ureters, converge at the exit from the bladder, and fuse to form a median urethral crest that continues into the pelvic urethra (Figure 5-34/5). The triangle bounded by the ureteric and urethral openings is termed the trigone; it appears to have a different origin from the remainder of the bladder wall (p. 169) and is believed to have an enhanced sensitivity (Figure 5-34/4). The bladder epithelium is of the transitional kind.
The bladder muscle is arranged in three sheets that exchange fascicles. The muscle is probably entirely detrusor—available to squeeze and empty the bladder— and fails to form an internal sphincter, although one is often described. Many now believe that, in place of this, some muscle bundles form a series of arcades whose summits are directed toward the orifice; they therefore dilate rather than occlude the exit when they contract. If this is so, continence depends on the tension passively
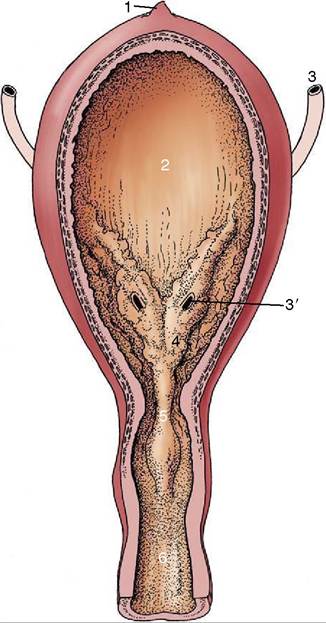
Figure 5-34 The interior of the urinary bladder. 1, Scar of urachus; 2, bladder; 3, ureter; 3'l ureteric orifice; 4, trigone of bladder; 5, urethral crest; 6, urethra.
exerted by the elastic elements within the mucosa and on the action of the external sphincter, the striated urethralis. This interpretation is consistent with the demonstration that in certain species (dog, goat) the proximal part of the urethra forms part of the urine reservoir, expanding as the bladder fills. The functional boundary between bladder and urethra would thus appear to be represented by the cranial limit of the urethralis in these species.
Autonomic fibers reach the bladder through the sympathetic hypogastric and parasympathetic pelvic nerves; the latter innervate the detrusor muscle. Sensory fibers are routed through the pudendal nerve. The main blood supply is from the vaginal (or prostatic) artery, but, as has been mentioned, it is supplemented by the reduced umbilical arteries.