» The Vertebral Canal
The relationships of the segments and cervical and lumbar enlargements of the spinal cord to the vertebrae are shown in Fig. 8.15. The first three sacral segments lie within the last lumbar vertebra, and the spinal cord terminates within the cranial quarter of the sacrum of the adult (Fig.
19.4).The meninges remain separate to a more caudal level than in other species, and there is still a substantial subarachnoid space at the lumbosacral level. A communication exists in this species between the lumbar part of the space and a local widening (ventriculus terminalis) of the central canal of the spinal cord.
Epidural Anesthesia: Both lumbosacral and caudal sites of injection are commonly employed to obtain epidural anesthesia. The procedure at the former level utilizes the divergence of the spinous process of the last lumbar and first sacral vertebrae for identification of the injection site (Fig. 19.4). Although the interarcuate space is quite large, its distance (8-10 cm) from the skin makes it relatively easy to miss. "Low" epidural anesthesia is performed between the first and second caudal vertebrae, where the site for injection is readily discovered by "pumping" the tail up and down. The needle is inserted with a cranial inclination so that its point enters the canal within the first tail vertebra.
The vascularization of the spinal cord is mainly through spinal branches of the vertebral artery and appears to be relevant to the etiology of a relatively frequent form of ataxia ("wobbles") that occurs in foals and young horses. This may have its origin in congenital malformation and subsequent exostoses of the cervical articular processes that narrow the cervical vertebral canal at the intervertebral levels. This narrowing exerts pressure on the cord, although it is said that the cord lesions might be secondary to interference with the venous drainage.
In this context, it should be known that the spinal arteries and veins are arranged in two sets, connected by relatively ineffectual anastomoses. One set of arteries and veins enters the cord by way of the ventral fissure and supplies (and drains) the central gray matter and a thin surrounding shell of white matter. The second set of arteries and veins passes over the lateral aspect to detach branches at intervals; these enter periodically to supply (and drain) the bulk of the white matter (Fig. 19.5). It is the veins of the second set that are supposedly compressed, leading to venous congestion and subsequent degeneration of the nervous tissue. It is claimed that the condition may develop in the fetus.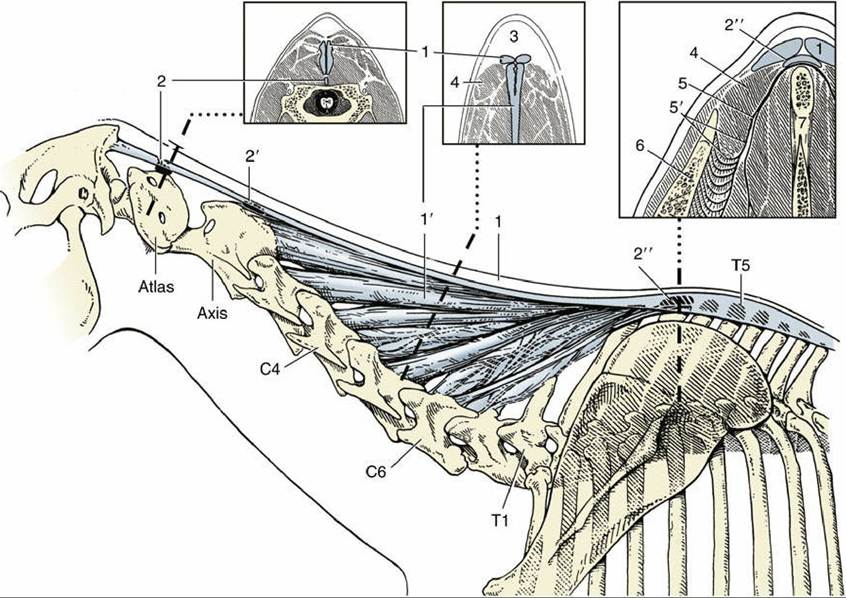
FIG. 19.3 The nuchal ligament and associated bursae in lateral view and in three transverse sections. 1 and 1', Funicular and laminar parts of nuchal ligament, respectively; 2, 2', and 2", cranial nuchal, caudal nuchal (inconstant), and supraspinous bursae, respectively; 3, fatty “crest” dorsal to nuchal ligament; 4, rhomboideus; 5, dorsoscapular ligament connecting spinous processes of the withers with the scapula; 5', elastic part of dorsoscapular ligament; 6, scapula; 7, spinous processes.
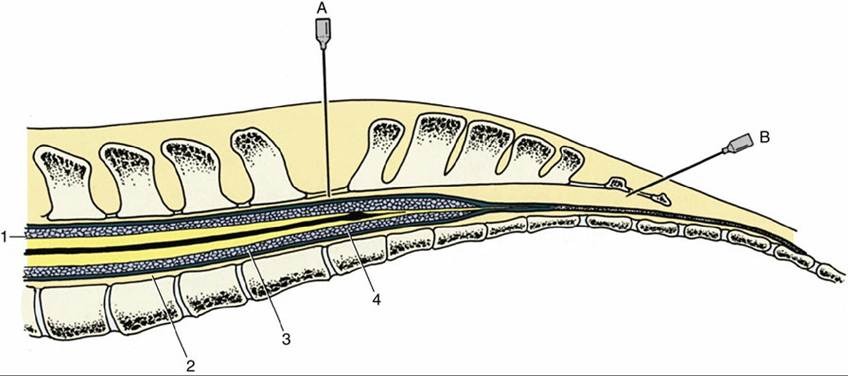
FIG. 19.4 Median section of the equine vertebral canal and spinal cord. The lumbosacral interarcuate space and the space between the first and second caudal vertebrae are indicated by hypodermic needles placed (A) for lumbosacral fluid collection and (B) for epidural anesthesia. 1, Pia mater; 2, dura mater; 3, arachnoid; 4, ventriculis terminalis.
Comprehension Check
Review the anatomy of the vertebral column, and determine with scientific reasoning the
appropriate sites for epidural injections.
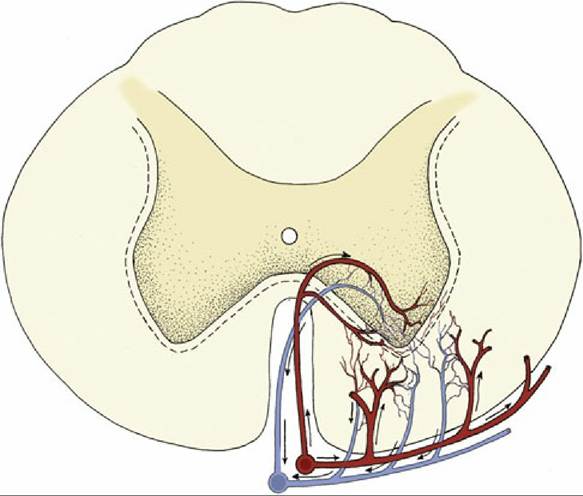
FIG. 19.5 Blood circulation in the ventral part of the spinal cord (schematic). The blood supply to the gray matter and to the adjacent layer of the white is more or less independent of that to most of the white matter.